Department of Medicine, University of California, San Francisco and Veterans Affairs Medical Center, San Francisco (R.S., C.G., M.G.S.). Division of Cardiology, Department of Medicine, Northwestern University Feinberg School of Medicine, Chicago, IL (S.J.S.). Division of Cardiology, Department of Medicine, Massachusetts General Hospital, Boston, MA (E.S.). Division of Cardiology, Department of Medicine, Stony Brook University, NY (J.B.). Department of Medicine, San Francisco General Hospital, University of California, San Francisco (P.Y.H.).
Circ Heart Fail. 2018 Apr;11(4):e004312. doi: 10.1161/CIRCHEARTFAILURE.117.004312.
Although individual cardiac biomarkers are associated with heart failure risk and all-cause mortality in HIV-infected individuals, their combined use for prediction has not been well studied.
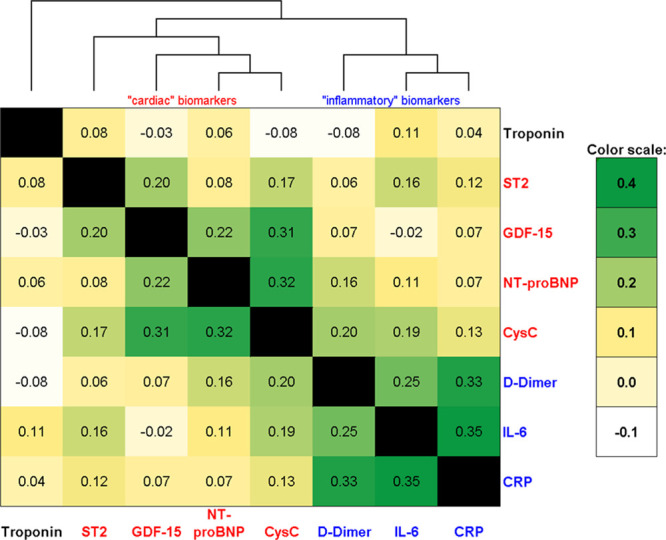
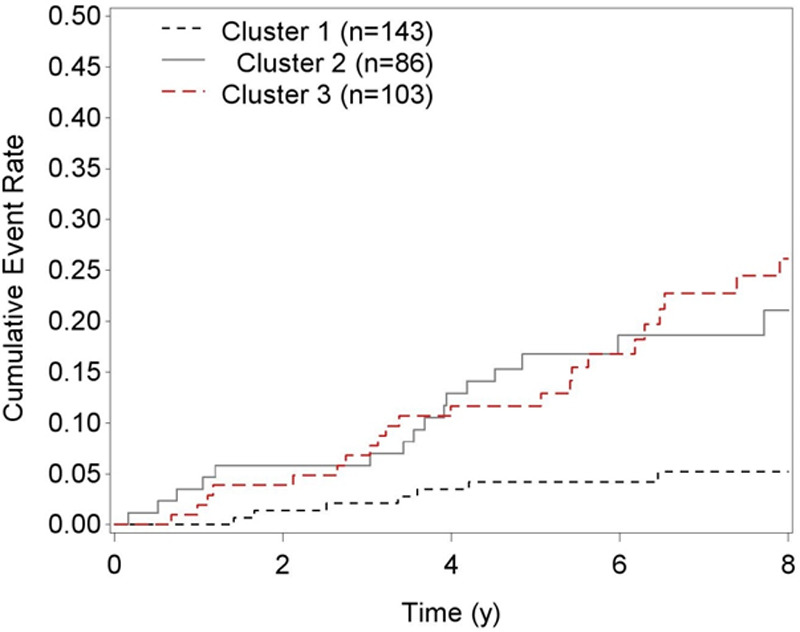
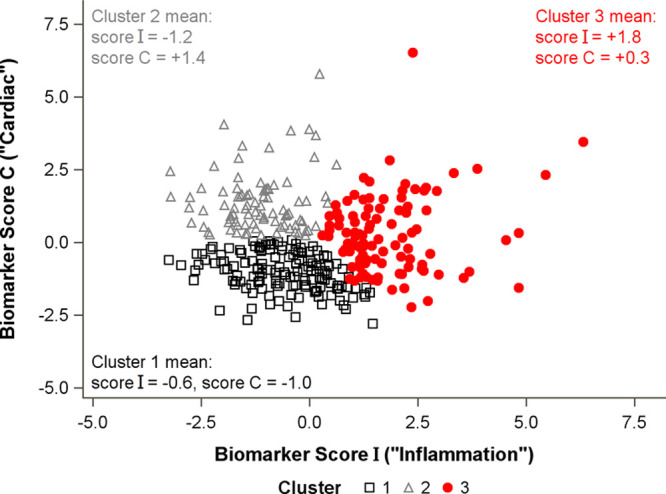
Unsupervised k-means cluster analysis was performed blinded to the study outcomes in 332 HIV-infected participants on 8 biomarkers: ST2, NT-proBNP (N-terminal pro-B-type natriuretic peptide), hsCRP (high-sensitivity C-reactive protein), GDF-15 (growth differentiation factor 15), cystatin C, IL-6 (interleukin-6), D-dimer, and troponin. We evaluated cross-sectional associations of each cluster with diastolic dysfunction, pulmonary hypertension (defined as echocardiographic pulmonary artery systolic pressure ≥35 mm Hg), and longitudinal associations with all-cause mortality. The biomarker-derived clusters partitioned subjects into 3 groups. Cluster 3 (n=103) had higher levels of CRP, IL-6, and D-dimer (inflammatory phenotype). Cluster 2 (n=86) displayed elevated levels of ST2, NT-proBNP, and GDF-15 (cardiac phenotype). Cluster 1 (n=143) had lower levels of both phenotype-associated biomarkers. After multivariable adjustment for traditional and HIV-related risk factors, cluster 3 was associated with a 51% increased risk of diastolic dysfunction (95% confidence interval, 1.12-2.02), and cluster 2 was associated with a 67% increased risk of pulmonary hypertension (95% confidence interval, 1.04-2.68), relative to cluster 1. Over a median 6.9-year follow-up, 48 deaths occurred. Cluster 3 was independently associated with a 3.3-fold higher risk of mortality relative to cluster 1 (95% confidence interval, 1.3-8.1), and cluster 2 had a 3.1-fold increased risk (95% confidence interval, 1.1-8.4), even after controlling for diastolic dysfunction, pulmonary hypertension, left ventricular mass, and ejection fraction.
Serum biomarkers can be used to classify HIV-infected individuals into separate clusters for differentiating cardiopulmonary structural and functional abnormalities and can predict mortality independent of these structural and functional measures.
虽然个别心脏生物标志物与 HIV 感染者的心力衰竭风险和全因死亡率相关,但它们在预测中的联合应用尚未得到充分研究。
在 332 名接受 8 种生物标志物(ST2、NT-proBNP(N 末端 pro-B 型利钠肽)、hsCRP(高敏 C 反应蛋白)、GDF-15(生长分化因子 15)、胱抑素 C、IL-6(白细胞介素-6)、D-二聚体和肌钙蛋白)检测的 HIV 感染者中,我们采用无监督 k-均值聚类分析,该分析对研究结果进行了盲法评估。我们评估了每个聚类与舒张功能障碍、肺动脉高压(定义为超声心动图肺动脉收缩压≥35mmHg)的横断面关联,以及与全因死亡率的纵向关联。生物标志物衍生的聚类将受试者分为 3 组。第 3 组(n=103)的 CRP、IL-6 和 D-二聚体水平较高(炎症表型)。第 2 组(n=86)显示 ST2、NT-proBNP 和 GDF-15 水平升高(心脏表型)。第 1 组(n=143)两种表型相关生物标志物水平较低。在对传统和 HIV 相关危险因素进行多变量调整后,与第 1 组相比,第 3 组舒张功能障碍的风险增加了 51%(95%置信区间,1.12-2.02),第 2 组肺动脉高压的风险增加了 67%(95%置信区间,1.04-2.68)。在中位 6.9 年的随访期间,有 48 人死亡。与第 1 组相比,第 3 组的死亡率独立增加了 3.3 倍(95%置信区间,1.3-8.1),第 2 组的死亡率增加了 3.1 倍(95%置信区间,1.1-8.4),即使在控制舒张功能障碍、肺动脉高压、左心室质量和射血分数后也是如此。
血清生物标志物可用于将 HIV 感染者分为不同的群组,以区分心肺结构和功能异常,并可预测死亡率,而与这些结构和功能测量无关。