Institute for Disease Modeling, Bellevue, Washington, USA.
Aurum Institute, Johannesburg, South Africa.
BMC Med. 2018 Apr 12;16(1):52. doi: 10.1186/s12916-018-1037-3.
Gold mines represent a potential hotspot for Mycobacterium tuberculosis (Mtb) transmission and may be exacerbating the tuberculosis (TB) epidemic in South Africa. However, the presence of multiple factors complicates estimation of the mining contribution to the TB burden in South Africa.
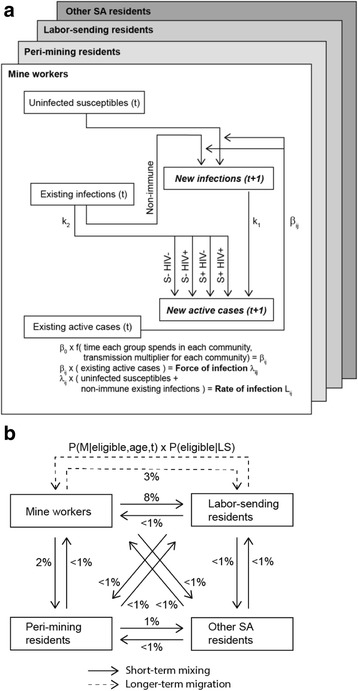
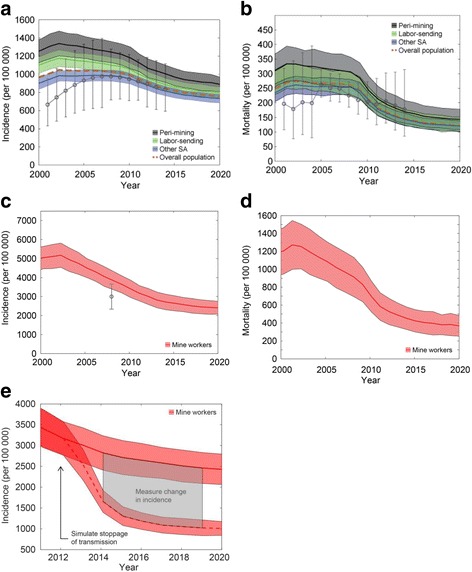
We developed two models of TB in South Africa, a static risk model and an individual-based model that accounts for longer-term trends. Both models account for four populations - mine workers, peri-mining residents, labor-sending residents, and other residents of South Africa - including the size and prevalence of latent TB infection, active TB, and HIV of each population and mixing between populations. We calibrated to mine- and country-level data and used the static model to estimate force of infection (FOI) and new infections attributable to local residents in each community compared to other residents. Using the individual-based model, we simulated a counterfactual scenario to estimate the fraction of overall TB incidence in South Africa attributable to recent transmission in mines.
We estimated that the majority of FOI in each community is attributable to local residents: 93.9% (95% confidence interval 92.4-95.1%), 91.5% (91.4-91.5%), and 94.7% (94.7-94.7%) in gold mining, peri-mining, and labor-sending communities, respectively. Assuming a higher rate of Mtb transmission in mines, 4.1% (2.6-5.8%), 5.0% (4.5-5.5%), and 9.0% (8.8-9.1%) of new infections in South Africa are attributable to gold mine workers, peri-mining residents, and labor-sending residents, respectively. Therefore, mine workers with TB disease, who constitute ~ 2.5% of the prevalent TB cases in South Africa, contribute 1.62 (1.04-2.30) times as many new infections as TB cases in South Africa on average. By modeling TB on a longer time scale, we estimate 63.0% (58.5-67.7%) of incident TB disease in gold mining communities to be attributable to recent transmission, of which 92.5% (92.1-92.9%) is attributable to local transmission.
Gold mine workers are estimated to contribute a disproportionately large number of Mtb infections in South Africa on a per-capita basis. However, mine workers contribute only a small fraction of overall Mtb infections in South Africa. Our results suggest that curtailing transmission in mines may have limited impact at the country level, despite potentially significant impact at the mining level.
金矿是结核分枝杆菌(Mycobacterium tuberculosis,Mtb)传播的潜在热点地区,可能使南非的结核病(tuberculosis,TB)流行更为严重。然而,多种因素的存在使得估算南非采矿业对结核病负担的影响变得复杂。
我们开发了南非结核病的两种模型,一种是静态风险模型,另一种是考虑到长期趋势的基于个体的模型。这两种模型都考虑了南非的四个人群——矿工、矿区周围居民、劳务输出居民和其他南非居民,包括每个人群的潜伏性结核感染、活动性结核和 HIV 的规模和流行率,以及人群之间的混合。我们根据矿区和国家层面的数据进行了校准,并使用静态模型来估算每个社区中归因于当地居民的局部感染率(force of infection,FOI)和新感染,与其他居民进行比较。使用基于个体的模型,我们模拟了一个反事实场景,以估算归因于南非矿山近期传播的总体结核病发病率的比例。
我们估计,每个社区的大部分 FOI 都归因于当地居民:金矿开采、矿区周围和劳务输出社区的 FOI 分别为 93.9%(95%置信区间为 92.4%-95.1%)、91.5%(91.4%-91.5%)和 94.7%(94.7%-94.7%)。假设矿山中结核分枝杆菌的传播率更高,南非的新感染分别归因于金矿工人、矿区周围居民和劳务输出居民的比例为 4.1%(2.6%-5.8%)、5.0%(4.5%-5.5%)和 9.0%(8.8%-9.1%)。因此,患有结核病的矿工占南非现有结核病病例的~2.5%,平均而言,他们导致的新感染比南非结核病病例多 1.62 倍(1.04-2.30)。通过对较长时间范围内的结核病进行建模,我们估计在金矿开采社区中,63.0%(58.5%-67.7%)的新发结核病病例归因于近期传播,其中 92.5%(92.1%-92.9%)归因于本地传播。
根据人均水平估计,南非金矿工人感染结核分枝杆菌的比例过高。然而,矿工对南非结核分枝杆菌感染的总人数只占很小的比例。我们的研究结果表明,尽管在矿山层面可能会产生重大影响,但在国家层面上,遏制矿山传播的效果可能有限。