Women's College Research Institute, 76 Grenville Street, Toronto, ON, M5S 1B1, Canada.
Institute of Medical Science, University of Toronto, Toronto, Canada.
Breast Cancer Res Treat. 2018 Aug;170(3):647-656. doi: 10.1007/s10549-018-4796-9. Epub 2018 Apr 24.
In patients with breast cancer, increasing tumour size at diagnosis is associated with an increased likelihood of axillary lymph node involvement and increased breast cancer-specific mortality. However, this relation is based on studies which combine all tumours smaller than 1.0 cm in a single category and all tumours larger than 5.0 cm in another category. This coarse classification may obscure a nuanced description of the effects of tumour size across the full range of possible sizes.
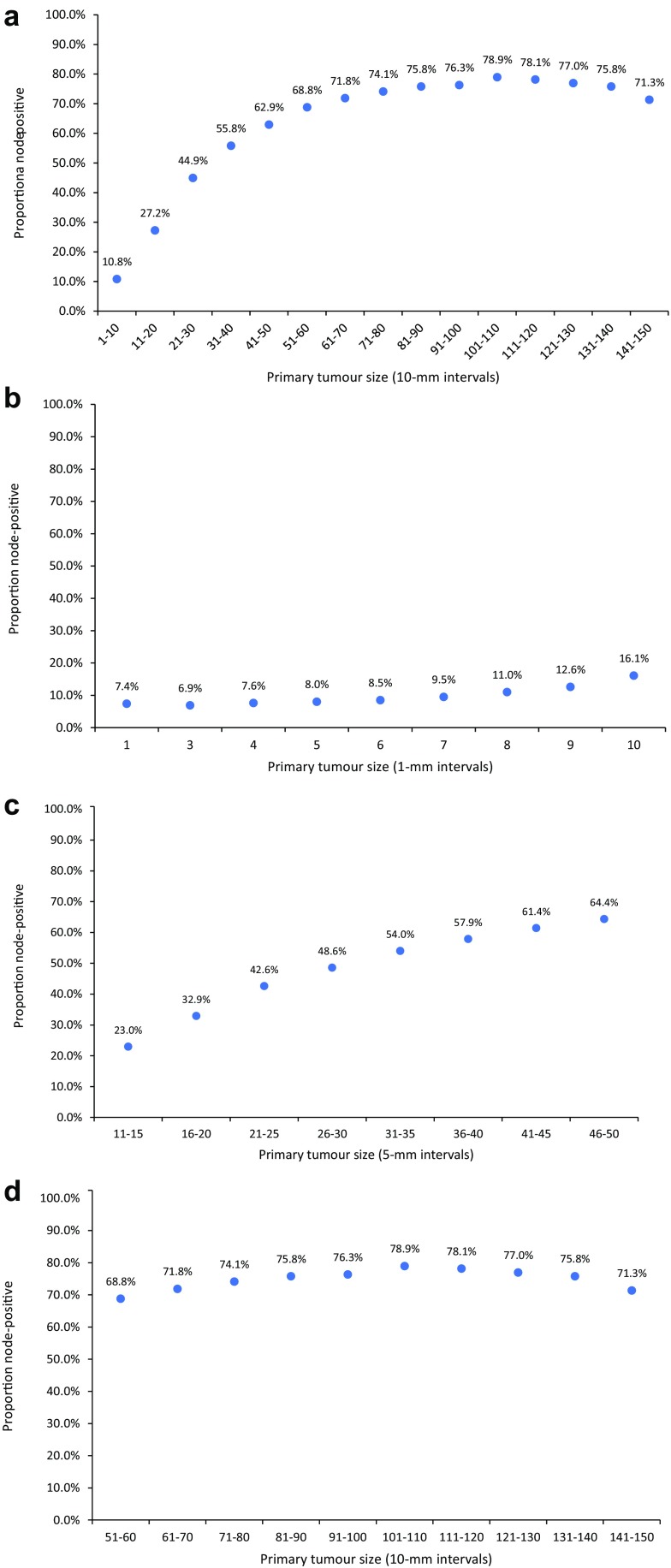
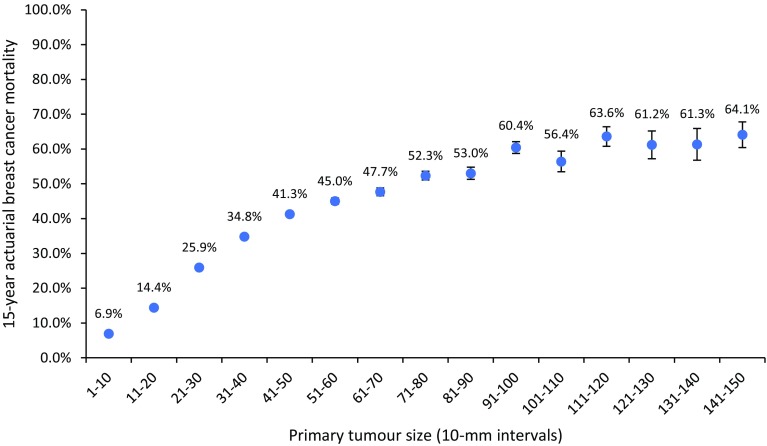
We examined the relationship between primary tumour size, lymph node status and distant metastases in a cohort of 819,647 women diagnosed with first primary invasive breast cancer from 1990 to 2014 in the Surveillance, Epidemiology and End Results (SEER) registries database. All patients in the cohort had a known primary tumour size between 1 and 150 mm in greatest dimension. Primary tumour size was examined as a continuous (1-150 mm) and categorical variable (15 size groups; 10-mm intervals). For each 1- or 10-mm size group, we determined the proportion of patients with positive lymph nodes at diagnosis, the proportion of patients with distant metastases at diagnosis and the actuarial cumulative risk of breast cancer-specific mortality at 15 years from diagnosis.
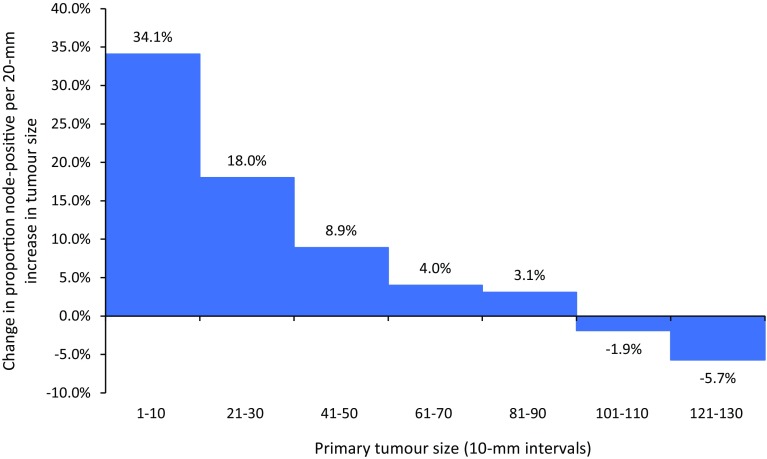
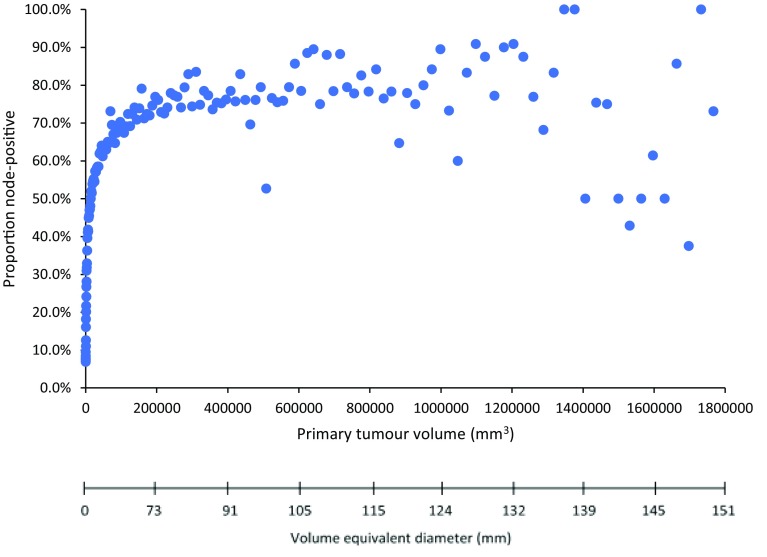
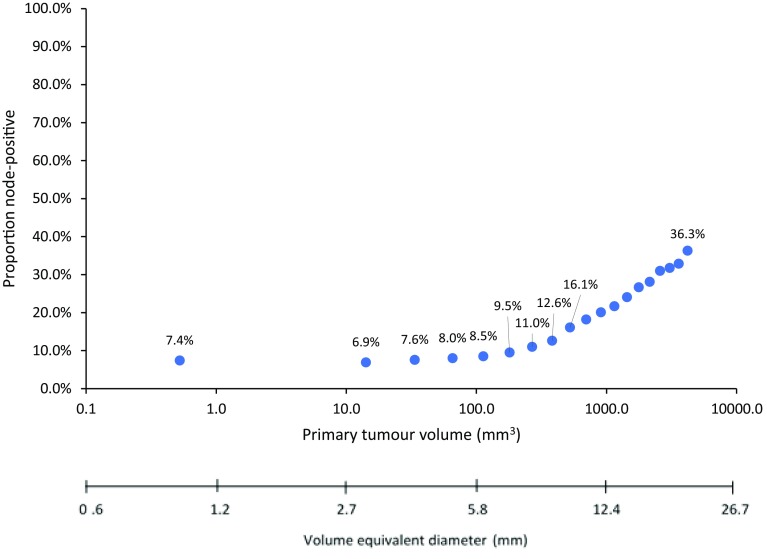
Among 819,647 patients with invasive breast tumours between 1 and 150 mm in size, there was a non-linear correlation between increasing tumour size and the prevalence of lymph node metastases at diagnosis (% node-positive), the prevalence of distant metastases at diagnosis (% stage IV) and the 15-year rate of breast cancer-specific mortality across the entire size spectrum. For very small tumours (under 10 mm) and for very large tumours (larger than 60-90 mm) there was little correlation between tumour size and metastasis risk.
The relationship between tumour size, lymph node status and distant metastases in patients with invasive breast cancer is not linear. This calls into question the conventional model that the capacity for a primary breast tumour to metastasize increases as the tumour enlarges.
在乳腺癌患者中,诊断时肿瘤大小的增加与腋窝淋巴结受累的可能性增加以及乳腺癌特异性死亡率增加相关。然而,这种关系是基于将所有小于 1.0 厘米的肿瘤组合在一个类别中和所有大于 5.0 厘米的肿瘤组合在另一个类别的研究。这种粗略的分类可能会掩盖肿瘤大小在整个可能范围内的影响的细致描述。
我们在 1990 年至 2014 年间,在监测、流行病学和最终结果(SEER)登记数据库中,检查了 819647 名被诊断为原发性浸润性乳腺癌的女性队列中,原发肿瘤大小、淋巴结状态和远处转移之间的关系。队列中的所有患者都有一个已知的原发肿瘤大小,在 1 至 150 毫米之间。原发肿瘤大小被视为连续变量(1-150 毫米)和分类变量(15 个大小组;10 毫米间隔)。对于每个 1 毫米或 10 毫米大小组,我们确定了诊断时淋巴结阳性患者的比例、诊断时远处转移患者的比例以及诊断后 15 年乳腺癌特异性死亡率的实际累积风险。
在 819647 名患有 1 至 150 毫米大小的浸润性乳腺肿瘤的患者中,在整个大小范围内,肿瘤大小的增加与诊断时淋巴结转移的流行率(%淋巴结阳性)、诊断时远处转移的流行率(%IV 期)和诊断后 15 年乳腺癌特异性死亡率呈非线性相关。对于非常小的肿瘤(小于 10 毫米)和非常大的肿瘤(大于 60-90 毫米),肿瘤大小与转移风险之间的相关性很小。
在患有浸润性乳腺癌的患者中,肿瘤大小、淋巴结状态和远处转移之间的关系不是线性的。这对肿瘤增大时原发性乳腺癌转移能力增加的传统模型提出了质疑。