Division of Gastroenterology/Hepatology, Department of Internal Medicine, Medical College of Georgia, Augusta University, Augusta, GA, USA.
Clin Transl Gastroenterol. 2018 Jun 19;9(6):162. doi: 10.1038/s41424-018-0030-7.
D-lactic acidosis is characterized by brain fogginess (BF) and elevated D-lactate and occurs in short bowel syndrome. Whether it occurs in patients with an intact gut and unexplained gas and bloating is unknown. We aimed to determine if BF, gas and bloating is associated with D-lactic acidosis and small intestinal bacterial overgrowth (SIBO).
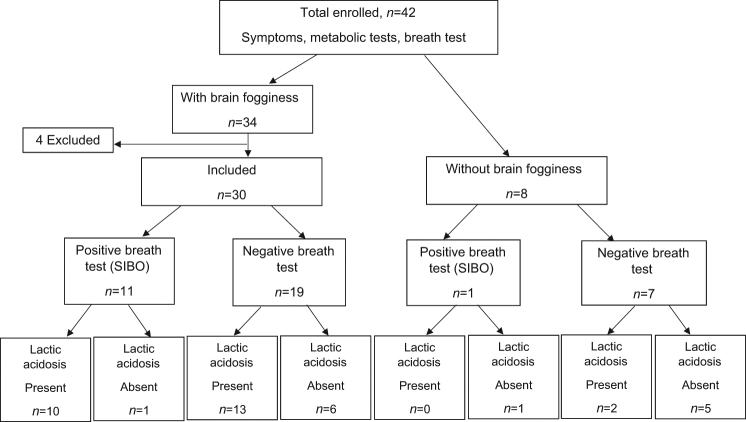
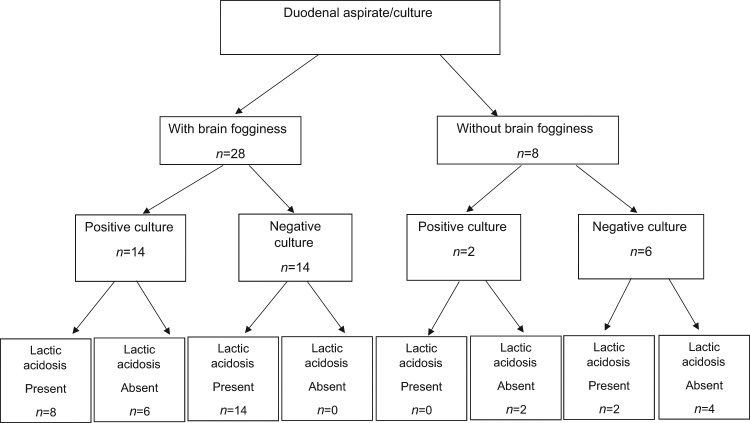
Patients with gas, bloating, BF, intact gut, and negative endoscopic and radiological tests, and those without BF were evaluated. SIBO was assessed with glucose breath test (GBT) and duodenal aspiration/culture. Metabolic assessments included urinary D-lactic acid and blood L-lactic acid, and ammonia levels. Bowel symptoms, and gastrointestinal transit were assessed.
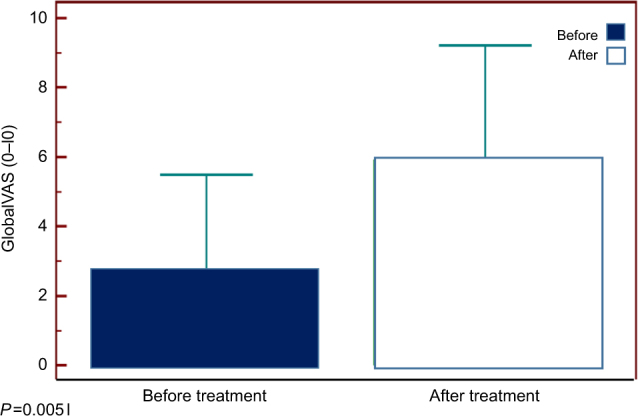
Thirty patients with BF and 8 without BF were evaluated. Abdominal bloating, pain, distension and gas were the most severe symptoms and their prevalence was similar between groups. In BF group, all consumed probiotics. SIBO was more prevalent in BF than non-BF group (68 vs. 28%, p = 0.05). D-lactic acidosis was more prevalent in BF compared to non-BF group (77 vs. 25%, p = 0.006). BF was reproduced in 20/30 (66%) patients. Gastrointestinal transit was slow in 10/30 (33%) patients with BF and 2/8 (25%) without. Other metabolic tests were unremarkable. After discontinuation of probiotics and a course of antibiotics, BF resolved and gastrointestinal symptoms improved significantly (p = 0.005) in 23/30 (77%).
We describe a syndrome of BF, gas and bloating, possibly related to probiotic use, SIBO, and D-lactic acidosis in a cohort without short bowel. Patients with BF exhibited higher prevalence of SIBO and D-lactic acidosis. Symptoms improved with antibiotics and stopping probiotics. Clinicians should recognize and treat this condition.
D-乳酸酸中毒的特点是脑雾(BF)和 D-乳酸升高,发生于短肠综合征。但在肠道完整且存在不明原因的气体和腹胀的患者中是否会发生,目前尚不清楚。我们旨在确定 BF、气体和腹胀是否与 D-乳酸酸中毒和小肠细菌过度生长(SIBO)有关。
评估了存在气体、腹胀、BF、肠道完整且内镜和影像学检查均为阴性,且不存在 BF 的患者。采用葡萄糖呼气试验(GBT)和十二指肠抽吸/培养来评估 SIBO。代谢评估包括尿 D-乳酸和血 L-乳酸及血氨水平。评估了肠道症状和胃肠道转运情况。
共评估了 30 例存在 BF 和 8 例不存在 BF 的患者。腹部饱胀、疼痛、腹胀和气体是最严重的症状,两组的发生率相似。在 BF 组中,所有患者均服用了益生菌。BF 组中 SIBO 的发生率高于非 BF 组(68%比 28%,p=0.05)。与非 BF 组相比,BF 组 D-乳酸酸中毒的发生率更高(77%比 25%,p=0.006)。在 30 例 BF 患者中有 20 例(66%)可重现 BF。在 30 例 BF 患者中有 10 例(33%)的胃肠道转运缓慢,而在 8 例非 BF 患者中只有 2 例(25%)。其他代谢检测结果无明显异常。停用益生菌并使用抗生素疗程后,BF 得到缓解,胃肠道症状明显改善(p=0.005),23 例(77%)患者的 BF 得到缓解。
我们描述了一种 BF、气体和腹胀的综合征,可能与益生菌使用、SIBO 和 D-乳酸酸中毒有关,而这些患者没有短肠。BF 患者 SIBO 和 D-乳酸酸中毒的发生率更高。症状改善与抗生素和停用益生菌有关。临床医生应认识并治疗这种情况。