Kyrios Michael, Ahern Claire, Fassnacht Daniel B, Nedeljkovic Maja, Moulding Richard, Meyer Denny
College of Education, Psychology & Social Work, Flinders University, Adelaide, Australia.
Research School of Psychology, The Australian National University, Canberra, Australia.
J Med Internet Res. 2018 Aug 8;20(8):e242. doi: 10.2196/jmir.9566.
Obsessive-compulsive disorder (OCD) is a highly disabling psychological disorder with a chronic course if left untreated. Cognitive behavioral therapy (CBT) has been shown to be an effective treatment, but access to face-to-face CBT is not always possible. Internet-based CBT (iCBT) has become an increasingly viable option. However, no study has compared iCBT to an analogous control condition using a randomized controlled trial (RCT).
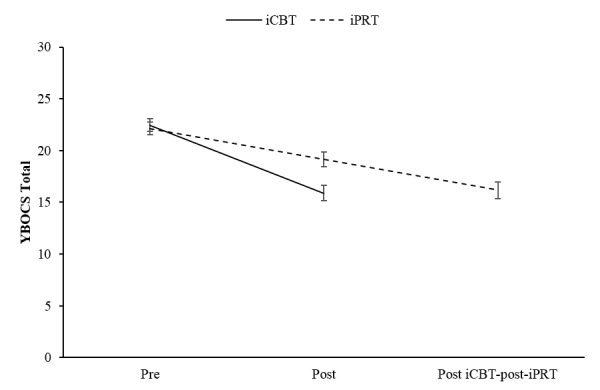
A 2-armed RCT was used to compare a therapist-assisted 12-module iCBT to an analogous active attention control condition (therapist-assisted internet-based standard progressive relaxation training, iPRT) in adult OCD. This paper reports pre-post findings for OCD symptom severity.
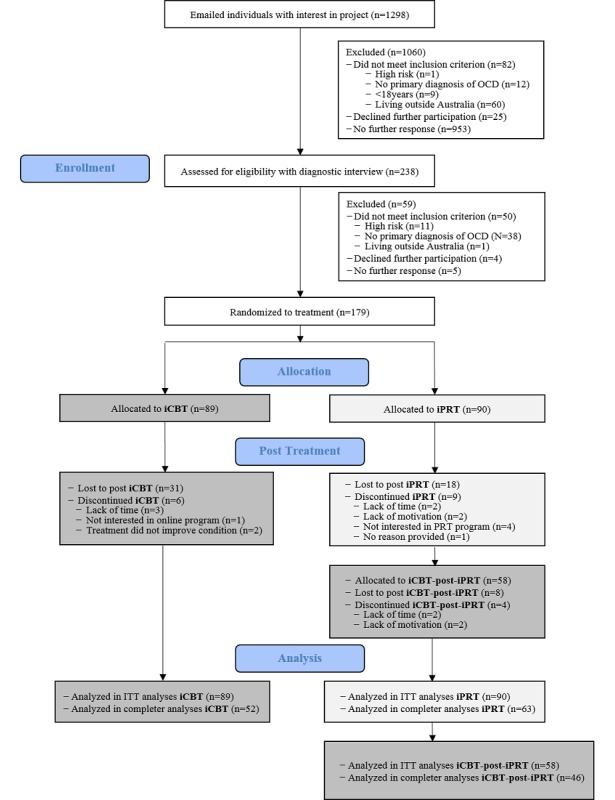
In total, 179 participants (117 females, 65.7%) were randomized (stratified by gender) into iCBT or iPRT. The iCBT intervention included psychoeducation, mood and behavioral management, exposure and response prevention (ERP), cognitive therapy, and relapse prevention; the iPRT intervention included psychoeducation and relaxation techniques as a way of managing OCD-related anxiety but did not incorporate ERP or other CBT elements. Both treatments included audiovisual content, case stories, demonstrations of techniques, downloadable audio content and worksheets, and expert commentary. All participants received 1 weekly email, with a maximum 15-minute preparation time per client from a remote therapist trained in e-therapy. Emails aimed to monitor progress, provide support and encouragement, and assist in individualizing the treatment. Participants were assessed for baseline and posttreatment OCD severity with the telephone-administered clinician-rated Yale-Brown Obsessive-Compulsive Scale and other measures by assessors who were blinded to treatment allocation.
No pretreatment differences were found between the 2 conditions. Intention-to-treat analysis revealed significant pre-post improvements in OCD symptom severity for both conditions (P<.001). However, relative to iPRT, iCBT showed significantly greater symptom severity improvement (P=.001); Cohen d for iCBT was 1.05 (95% CI 0.72-1.37), whereas for iPRT it was 0.48 (95% CI 0.22-0.73). The iCBT condition was superior in regard to reliable improvement (25/51, 49% vs 16/55, 29%; P=.04) and clinically significant pre-post-treatment changes (17/51, 33% vs 6/55, 11%; P=.005). Those undertaking iCBT post completion of iPRT showed further significant symptom amelioration (P<.001), although the sequential treatment was no more efficacious than iCBT alone (P=.63).
This study is the first to compare a therapist-assisted iCBT program for OCD to an analogous active attention control condition using iPRT. Our findings demonstrate the large magnitude effect of iCBT for OCD; interestingly, iPRT was also moderately efficacious, albeit significantly less so than the iCBT intervention. The findings are compared to previous internet-based and face-to-face CBT treatment programs for OCD. Future directions for technology-enhanced programs for the treatment of OCD are outlined.
Australian New Zealand Clinical Trials Registry ACTRN12611000321943; https://www.anzctr.org.au/Trial/Registration/TrialReview.aspx?id=336704 (Archived by WebCite at http://www.webcitation.org/70ovUiOmd).
强迫症(OCD)是一种严重致残的心理障碍,若不治疗会呈慢性病程。认知行为疗法(CBT)已被证明是一种有效的治疗方法,但并非总能获得面对面的CBT治疗。基于互联网的CBT(iCBT)已成为越来越可行的选择。然而,尚无研究使用随机对照试验(RCT)将iCBT与类似的对照条件进行比较。
采用双臂RCT比较成人强迫症患者中治疗师辅助的12模块iCBT与类似的积极注意力控制条件(治疗师辅助的基于互联网的标准渐进性放松训练,iPRT)。本文报告强迫症症状严重程度的前后结果。
总共179名参与者(117名女性,65.7%)被随机分组(按性别分层)进入iCBT或iPRT组。iCBT干预包括心理教育、情绪和行为管理、暴露与反应阻止(ERP)、认知疗法以及复发预防;iPRT干预包括心理教育和放松技巧,作为管理与强迫症相关焦虑的一种方式,但未纳入ERP或其他CBT要素。两种治疗均包括视听内容、案例故事、技巧演示、可下载音频内容和工作表以及专家评论。所有参与者每周收到1封电子邮件,远程接受电子治疗培训的治疗师为每位客户准备时间最长15分钟。电子邮件旨在监测进展、提供支持和鼓励,并协助个性化治疗。通过电话管理的临床医生评定的耶鲁-布朗强迫症量表和其他测量方法,由对治疗分配不知情的评估人员对参与者的强迫症严重程度进行基线和治疗后评估。
两种条件在治疗前未发现差异。意向性分析显示两种条件下强迫症症状严重程度在治疗前后均有显著改善(P<.001)。然而,相对于iPRT,iCBT显示出症状严重程度改善显著更大(P=.001);iCBT的Cohen d为1.05(95%CI 0.72 - 1.37),而iPRT为0.48(95%CI 0.22 - 0.73)。iCBT组在可靠改善方面更优(25/51,49%对16/55,29%;P=.04)以及治疗前后具有临床显著变化方面更优(17/51,33%对6/55,11%;P=.005)。在完成iPRT后进行iCBT的患者症状进一步显著改善(P<.001),尽管序贯治疗并不比单独的iCBT更有效(P=.63)。
本研究首次将治疗师辅助的强迫症iCBT项目与使用iPRT的类似积极注意力控制条件进行比较。我们的研究结果证明了iCBT对强迫症的显著效果;有趣的是,iPRT也有一定疗效,尽管明显低于iCBT干预。将这些结果与先前针对强迫症的基于互联网和面对面的CBT治疗项目进行了比较。概述了技术增强型强迫症治疗项目的未来方向。
澳大利亚新西兰临床试验注册中心ACTRN12611000321943;https://www.anzctr.org.au/Trial/Registration/TrialReview.aspx?id=336704(由WebCite存档于http://www.webcitation.org/70ovUiOmd)