Martí-Pastor Marc, Pont Angels, Ávila Mónica, Garin Olatz, Vilagut Gemma, Forero Carlos G, Pardo Yolanda, Tresserras Ricard, Medina-Bustos Antonia, Garcia-Codina Oriol, Cabasés Juan, Rajmil Luis, Alonso Jordi, Ferrer Montse
IMIM (Hospital del Mar Medical Research Institute), Health Services Research Group, Doctor Aiguader, 88, 08003, Barcelona, Spain.
CIBER en Epidemiología y Salud Pública (CIBERESP), Madrid, Spain.
Popul Health Metr. 2018 Aug 16;16(1):14. doi: 10.1186/s12963-018-0170-8.
The EQ-5D has been frequently used in national health surveys. This study is a head-to-head comparison to assess how expanding the number of levels from three (EQ-5D-3L) to five in the new EQ-5D-5L version has improved its distribution, discriminatory power, and validity in the general population.
A representative sample (N = 7554) from the Catalan Health Interview Survey 2011-2012, aged ≥18, answered both EQ-5D versions, and we evaluated the response redistribution and inconsistencies between them. To assess validity of this redistribution, we calculated the mean of the Visual Analogue Scale (VAS), which measures perceived health. The discriminatory power was examined with Shannon Indices, calculated for each dimension separately. Spanish preference value sets were applied to obtain utility indices, examining their distribution with statistics of central tendency and dispersion. We estimated the proportion of individuals reporting the best health state in EQ-5D-5L and EQ-5D-3L within groups of specific chronic conditions and their VAS mean.
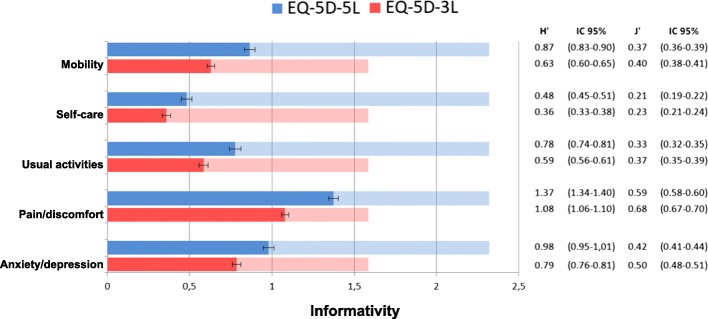
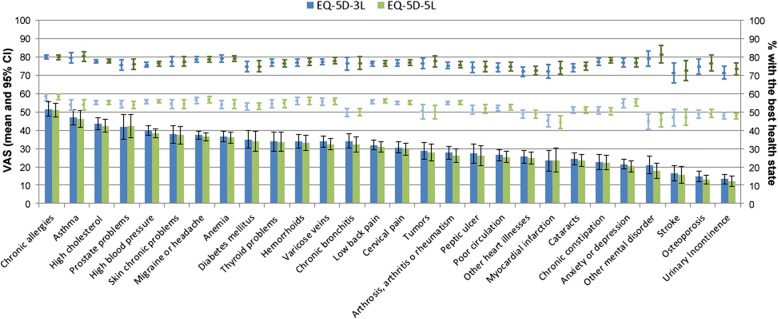
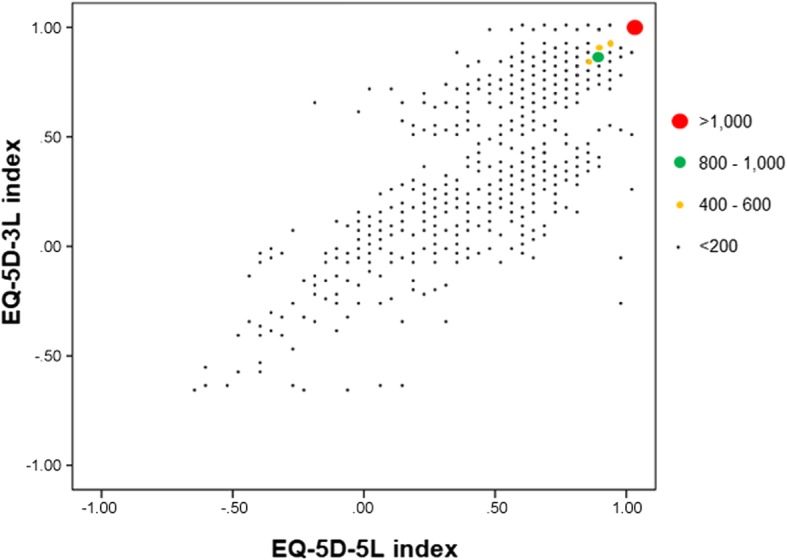
A very small reduction in the percentage of individuals with the best health state was observed, from 61.8% in EQ-5D-3L to 60.8% in EQ-5D-5L. In contrast, a large proportion of individuals reporting extreme problems in the 3 L version moved to severe problems (level 4) in the 5 L version, particularly for pain/discomfort (75.5%) and anxiety/depression (66.4%). The average proportion of inconsistencies was 0.9%. The pattern of the perceived health VAS mean confirmed the hypothesis established a priori, supporting the validity of the observed redistribution. Shannon index showed that absolute informativity was higher in the 5 L version for all dimensions. The means (SD) of the Spanish EQ-5D-3L and EQ-5D-5L indices were 0.87 (0.25) and 0.89 (0.22). The proportion of individuals with the best health state within each specific chronic condition was very similar, regardless of the EQ-5D version (≤ 30% in half of the 28 chronic conditions).
Although the proportion of individuals with the best possible health state is still very high, our findings support that the increase of levels provided by the EQ-5D-5L contributed to the validity and discriminatory power of this new version to measure health in general population, as in the national health surveys.
EQ-5D已在全国健康调查中频繁使用。本研究进行了直接比较,以评估将新版EQ-5D-5L从三个等级(EQ-5D-3L)扩展到五个等级如何改善了其在普通人群中的分布、区分能力和效度。
从2011 - 2012年加泰罗尼亚健康访谈调查中选取年龄≥18岁的代表性样本(N = 7554),让他们回答两个版本的EQ-5D,我们评估了两者之间的回答重新分布情况和不一致性。为评估这种重新分布的效度,我们计算了视觉模拟量表(VAS)的均值,该量表用于衡量自我感知健康状况。通过分别为每个维度计算香农指数来检验区分能力。应用西班牙偏好值集来获得效用指数,并用集中趋势和离散度统计量来检验其分布。我们估计了在特定慢性病组中报告EQ-5D-5L和EQ-5D-3L中最佳健康状态的个体比例及其VAS均值。
观察到报告最佳健康状态的个体百分比有非常小的下降,从EQ-5D-3L中的61.8%降至EQ-5D-5L中的60.8%。相比之下,大量在3L版本中报告极端问题的个体在5L版本中变为严重问题(4级),尤其是在疼痛/不适(75.5%)和焦虑/抑郁(66.4%)方面。不一致的平均比例为0.9%。自我感知健康VAS均值的模式证实了先验设定的假设,支持了所观察到的重新分布的效度。香农指数表明,5L版本在所有维度上的绝对信息量都更高。西班牙EQ-5D-3L和EQ-5D-5L指数的均值(标准差)分别为0.87(0.25)和0.89(0.22)。无论EQ-5D版本如何,每种特定慢性病中报告最佳健康状态的个体比例都非常相似(在28种慢性病中的半数中≤30%)。
尽管报告最佳健康状态的个体比例仍然非常高,但我们的研究结果支持,EQ-5D-5L增加的等级有助于该新版本在测量普通人群健康状况时的效度和区分能力,就像在全国健康调查中一样。