Klotz Daniel, Jansen Stefanie, Gebauer Corinna, Fuchs Hans
Department of Neonatology, Center for Pediatrics, Medical Center - University of Freiburg, Faculty of Medicine, University of Freiburg, Freiburg, Germany.
Department of Neonatology, University Children's Hospital, Leipzig, Germany.
Front Pediatr. 2018 Sep 4;6:235. doi: 10.3389/fped.2018.00235. eCollection 2018.
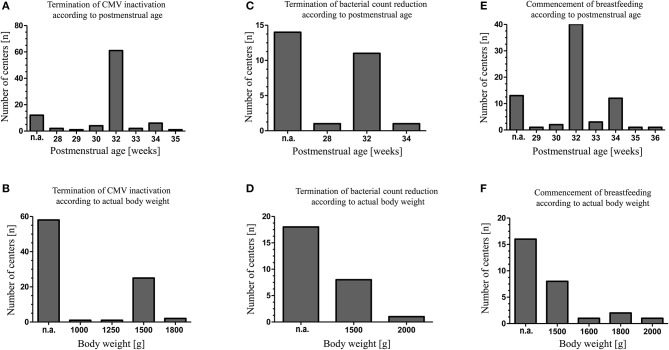
Breast milk (BM) for premature infants is subjected to multiple steps of processing, storage and distribution. These steps may influence the quality and safety of BM. Guidelines concerning the use of mother's own milk are either not available or limited to specific aspects of BM handling and are based on evidence of variable strength. This may result in diverse BM handling routines by health care professionals. We surveyed neonatal units to increase the knowledge about the current practice of BM handling routines of mother's own milk and to identify controversial aspects that could give directions for future research. An online-based questionnaire was sent to 307 different neonatal departments providing level III to level I neonatal care within Germany, Austria and Switzerland. Practices concerning screening for cytomegalovirus and BM bacteria, pasteurization, fortification, storage, workforce and the incidence of BM administration errors were surveyed. A total of 152 units, 56% of contacted level III units and 51% of level II units, participated in the survey (Germany 53%, Switzerland 71%, and Austria 56%). We found differences concerning indication and method of CMV inactivation (performed by 58%), bacterial count screening (48%) and bacterial count reduction (17%) within participating units. Thirty different thresholds for bacterial BM counts were reported by 65 units, resulting in pasteurization or discarding of BM. The use of nutrient analysis (12%) and fortification regimens in addition to standard multicomponent fortifiers (58%) using either individual (93%), targeted (3%), or adjusted (4%) fortification protocols varied profoundly. There is a high variability in staff and available facilities for BM handling. 73% of units report about BM administration errors. There is a wide variability in most aspects of BM handling in the participating units. Despite limited evidence labor and cost intensive procedures are applied which may have an impact on BM quality.
早产儿母乳要经过多个加工、储存和分发步骤。这些步骤可能会影响母乳的质量和安全性。关于使用母亲自身母乳的指南要么不存在,要么仅限于母乳处理的特定方面,且基于强度不一的证据。这可能导致医护人员采用不同的母乳处理常规。我们对新生儿病房进行了调查,以增加对母亲自身母乳处理常规当前做法的了解,并确定可能为未来研究指明方向的有争议方面。向德国、奥地利和瑞士境内提供三级到一级新生儿护理的307个不同新生儿科室发送了一份在线问卷。调查了有关巨细胞病毒和母乳细菌筛查、巴氏消毒、强化、储存、工作人员以及母乳给药错误发生率的做法。共有152个科室参与了调查,占所联系三级科室的56%和二级科室的51%(德国为53%,瑞士为71%,奥地利为56%)。我们发现参与调查的科室在巨细胞病毒灭活的指征和方法(58%的科室进行)、细菌计数筛查(48%)和细菌计数减少(17%)方面存在差异。65个科室报告了30种不同的母乳细菌计数阈值,导致母乳进行巴氏消毒或丢弃。除标准多成分强化剂外,使用营养分析的情况(12%)以及使用个体(93%)、靶向(3%)或调整(4%)强化方案的强化方案(58%)差异很大。母乳处理的工作人员和可用设施存在很大差异。73%的科室报告了母乳给药错误。参与调查的科室在母乳处理的大多数方面存在很大差异。尽管证据有限,但仍采用了 labor and cost intensive procedures,这可能会对母乳质量产生影响。 (注:“labor and cost intensive procedures”这里原文表述似乎有误,推测可能是“labor- and cost-intensive procedures”,意为劳动和成本密集型程序 )