Research Department, Reha Rheinfelden, Rheinfelden, Switzerland.
Institute for Rehabilitation and Performance Technology, Bern University of Applied Sciences, Burgdorf, Switzerland.
PLoS One. 2018 Oct 24;13(10):e0204455. doi: 10.1371/journal.pone.0204455. eCollection 2018.
Virtual reality-based training has found increasing use in neurorehabilitation to improve upper limb training and facilitate motor recovery.
The aim of this study was to directly compare virtual reality-based training with conventional therapy.
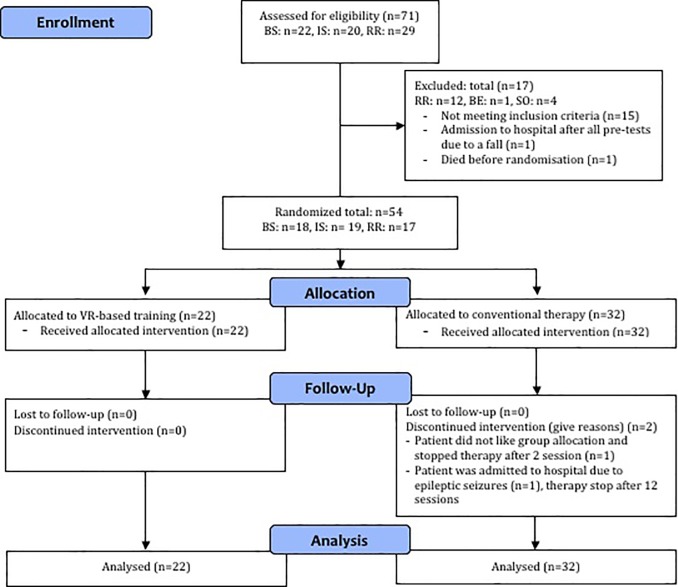
In a multi-center, parallel-group randomized controlled trial, patients at least 6 months after stroke onset were allocated either to an experimental group (virtual reality-based training) or a control group receiving conventional therapy (16x45 minutes within 4 weeks). The virtual reality-based training system replicated patients´ upper limb movements in real-time to manipulate virtual objects. Blinded assessors tested patients twice before, once during, and twice after the intervention up to 2-month follow-up for dexterity (primary outcome: Box and Block Test), bimanual upper limb function (Chedoke-McMaster Arm and Hand Activity Inventory), and subjective perceived changes (Stroke Impact Scale).
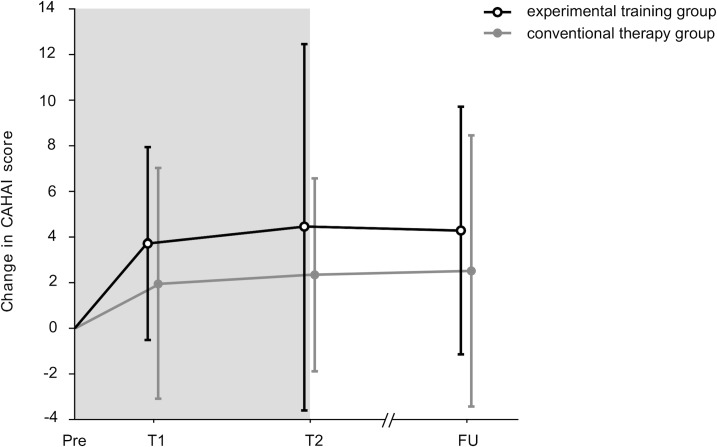
54 eligible patients (70 screened) participated (15 females, mean age 61.3 years, range 20-81 years, time since stroke 3.0±SD 3 years). 22 patients were allocated to the experimental group and 32 to the control group (3 drop-outs). Patients in the experimental and control group improved: Box and Block Test mean 21.5±SD 16 baseline to mean 24.1±SD 17 follow-up; Chedoke-McMaster Arm and Hand Activity Inventory mean 66.0±SD 21 baseline to mean 70.2±SD 19 follow-up. An intention-to-treat analysis found no between-group differences.
Patients in the experimental and control group showed similar effects, with most improvements occurring in the first two weeks and persisting until the end of the two-month follow-up period. The study population had moderate to severely impaired motor function at entry (Box and Block Test mean 21.5±SD 16). Patients, who were less impaired (Box and Block Test range 18 to 72) showed higher improvements in favor of the experimental group. This result could suggest that virtual reality-based training might be more applicable for such patients than for more severely impaired patients.
ClinicalTrials.gov NCT01774669.
基于虚拟现实的训练在神经康复中得到了越来越多的应用,以改善上肢训练和促进运动功能恢复。
本研究旨在直接比较基于虚拟现实的训练与常规治疗。
在一项多中心、平行组随机对照试验中,至少在中风后 6 个月的患者被分配到实验组(基于虚拟现实的训练)或对照组(在 4 周内接受 16 次 45 分钟的常规治疗)。基于虚拟现实的训练系统实时复制患者的上肢运动,以操纵虚拟物体。在干预前、干预期间和干预后 2 个月的随访中,盲法评估员对患者进行了两次测试,用于测试灵巧性(主要结果:箱式和区块测试)、双手上肢功能(切多克-麦克马斯特上肢活动量表)和主观感知变化(中风影响量表)。
54 名符合条件的患者(70 名筛选)参与了研究(15 名女性,平均年龄 61.3 岁,范围 20-81 岁,中风后时间 3.0±SD 3 年)。22 名患者被分配到实验组,32 名患者被分配到对照组(3 名退出)。实验组和对照组的患者均有所改善:箱式和区块测试平均 21.5±SD 16 基线到平均 24.1±SD 17 随访;切多克-麦克马斯特上肢活动量表平均 66.0±SD 21 基线到平均 70.2±SD 19 随访。意向治疗分析发现组间无差异。
实验组和对照组的患者均显示出相似的效果,大多数改善发生在最初的两周内,并持续到两个月随访期结束。研究人群的运动功能在进入研究时就已经受损(箱式和区块测试平均 21.5±SD 16)。功能受损程度较低(箱式和区块测试范围 18 到 72)的患者对实验组的改善效果更高。这一结果表明,基于虚拟现实的训练可能更适用于此类患者,而不是更严重受损的患者。
ClinicalTrials.gov NCT01774669。