Esaiassen Eirin, Hjerde Erik, Cavanagh Jorunn Pauline, Pedersen Tanja, Andresen Jannicke H, Rettedal Siren I, Støen Ragnhild, Nakstad Britt, Willassen Nils P, Klingenberg Claus
Paediatric Research Group, Department of Clinical Medicine, UiT The Arctic University of Norway, Tromsø, Norway.
Department of Paediatrics, University Hospital of North Norway, Tromsø, Norway.
Front Pediatr. 2018 Nov 16;6:347. doi: 10.3389/fped.2018.00347. eCollection 2018.
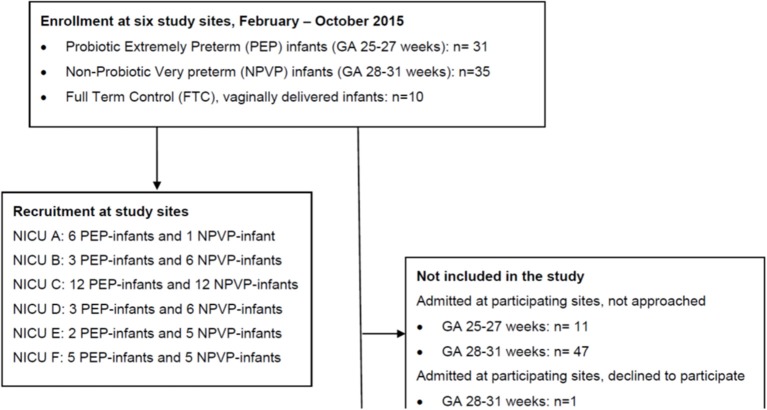
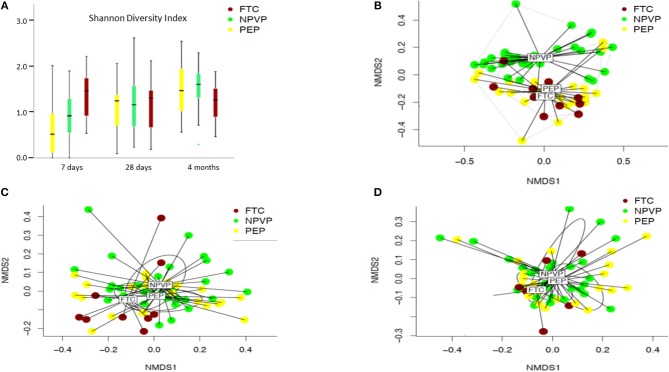
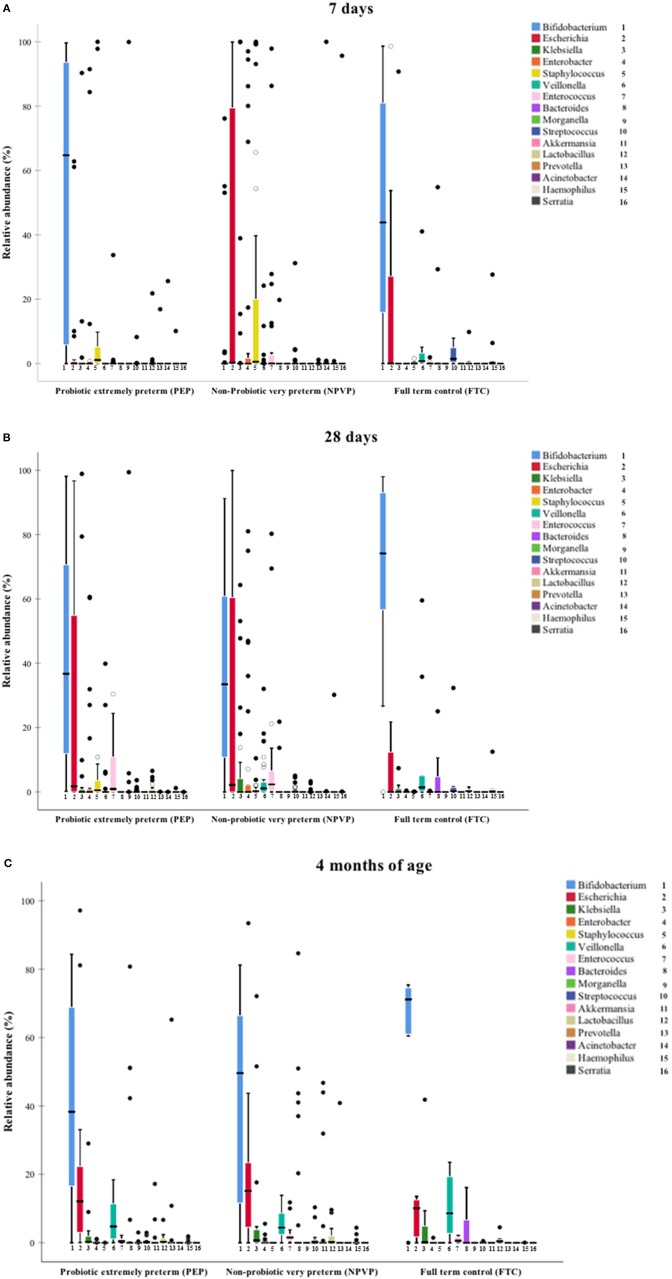
In 2014 probiotic supplementation ( and subspecies Infloran) was introduced as standard of care to prevent necrotizing enterocolitis (NEC) in extremely preterm infants in Norway. We aimed to evaluate the influence of probiotics and antibiotic therapy on the developing gut microbiota and antibiotic resistome in extremely preterm infants, and to compare with very preterm infants and term infants not given probiotics. A prospective, observational multicenter study in six tertiary-care neonatal units. We enrolled 76 infants; 31 probiotic-supplemented extremely preterm infants <28 weeks gestation, 35 very preterm infants 28-31 weeks gestation not given probiotics and 10 healthy full-term control infants. Taxonomic composition and collection of antibiotic resistance genes (resistome) in fecal samples, collected at 7 and 28 days and 4 months age, were analyzed using shotgun-metagenome sequencing. Median (IQR) birth weight was 835 (680-945) g and 1,290 (1,150-1,445) g in preterm infants exposed and not exposed to probiotics, respectively. Two extremely preterm infants receiving probiotic developed NEC requiring surgery. At 7 days of age we found higher median relative abundance of in probiotic supplemented infants (64.7%) compared to non-supplemented preterm infants (0.0%) and term control infants (43.9%). was only detected in small amounts in all groups, but the relative abundance increased up to 4 months. Extremely preterm infants receiving probiotics had also much higher antibiotic exposure, still overall microbial diversity and resistome was not different than in more mature infants at 4 weeks and 4 months. Probiotic supplementation may induce colonization resistance and alleviate harmful effects of antibiotics on the gut microbiota and antibiotic resistome. Clinicaltrials.gov: NCT02197468. https://clinicaltrials.gov/ct2/show/NCT02197468.
2014年,挪威将补充益生菌(及亚种Infloran)作为极早产儿预防坏死性小肠结肠炎(NEC)的标准治疗方法。我们旨在评估益生菌和抗生素治疗对极早产儿肠道微生物群发育及抗生素耐药基因组的影响,并与未使用益生菌的极早产儿和足月儿进行比较。这是一项在六个三级护理新生儿病房开展的前瞻性观察性多中心研究。我们纳入了76名婴儿;31名补充益生菌的孕龄小于28周的极早产儿、35名孕龄28 - 31周未补充益生菌的极早产儿以及10名健康足月儿作为对照。使用鸟枪法宏基因组测序分析在7天、28天及4个月龄时采集的粪便样本中的分类组成及抗生素耐药基因(耐药基因组)。暴露于益生菌和未暴露于益生菌的早产儿的出生体重中位数(四分位间距)分别为835(680 - 945)克和1,290(1,150 - 1,445)克。两名接受益生菌治疗的极早产儿发生了需要手术的NEC。在7日龄时,我们发现补充益生菌的婴儿中[具体细菌名称未给出]的相对丰度中位数较高(64.7%),相比之下,未补充益生菌的早产儿(0.0%)和足月儿对照组(43.9%)较低。[具体细菌名称未给出]在所有组中仅少量检测到,但其相对丰度在4个月时有所增加。接受益生菌治疗的极早产儿的抗生素暴露也更高,但在4周和4个月时,其总体微生物多样性和耐药基因组与更成熟的婴儿并无差异。补充益生菌可能诱导定植抗性,并减轻抗生素对肠道微生物群和抗生素耐药基因组的有害影响。Clinicaltrials.gov:NCT02197468。https://clinicaltrials.gov/ct2/show/NCT02197468 。