Hospital Universitario Dr. José Eleuterio González, Universidad Autónoma de Nuevo León, Monterrey, Nuevo León, Mexico.
Laboratorio de Resistencia Bacteriana; Centro de Investigación Sobre Enfermedades Infecciosas, Instituto Nacional de Salud Pública, Cuernavaca, Morelos, Mexico.
PLoS One. 2019 Feb 13;14(2):e0209609. doi: 10.1371/journal.pone.0209609. eCollection 2019.
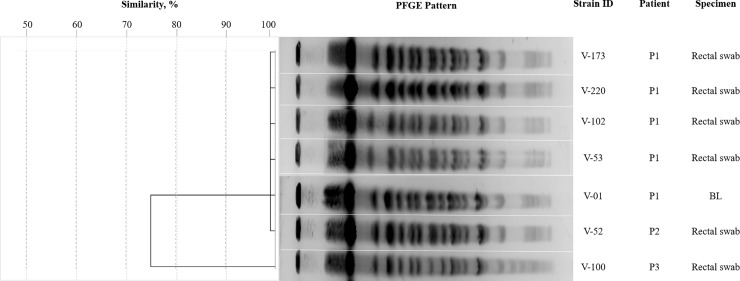
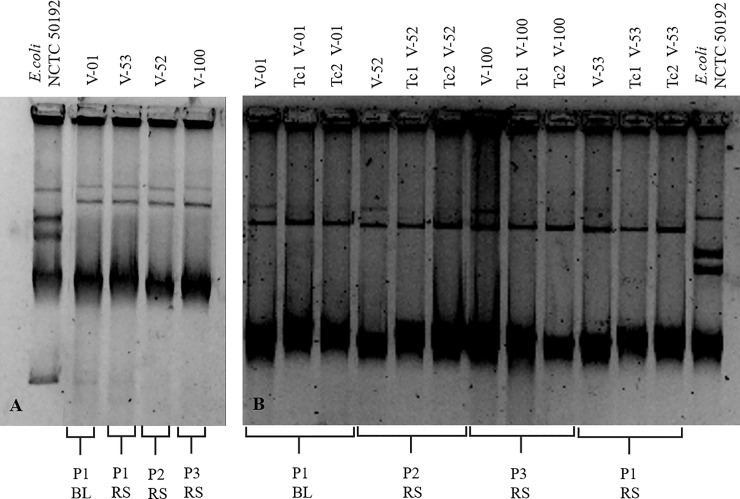
The worldwide dissemination of high-risk carbapenemase-producing Klebsiella pneumoniae clones has become a major threat to healthcare facilities. This study describes the successful containment of a hospital outbreak caused by NDM-1-producing K. pneumoniae Sequence Type (ST) 307 using active surveillance. The outbreak began when a patient was transferred from a local hospital. After 48 hours in our hospital, a tracheal aspirate was positive for a meropenem resistant and carbapenemase-producing K. pneumoniae. All patients in the medical intensive care unit (ICU) and the neurology wards were subject to contact precautions. The hospital surfaces and devices, healthcare workers, and patients from these wards were screened by cultures. Fecal swabs were placed into broth and PCR for blaKPC, blaOXA-48, blaIMP, blaVIM, and blaNDM, which were performed directly from the broth after 12 hours. PCRs were also performed on DNA extracted from carbapenemase-producing species from subcultured broths. Five and nine days later, two more patients' rectal swabs tested positive. Molecular assays identified K. pneumoniae blaNDM-1 onto a 130-kb conjugative plasmid (IncY, IncFIIs, and IncFIIY), ST307. After the three patients were discharged, monitoring continued, and after three weeks with negative results, rectal swabbing ended. In conclusion, it was possible to contain a hospital outbreak caused by NDM-1-producing K. pneumoniae ST307 through epidemiological and microbiological surveillance. With the methodology used, the detection of NDM-type genes in fecal samples was obtained in approximately 15 hours after obtaining the fecal sample.
产高风险碳青霉烯酶肺炎克雷伯菌克隆的全球传播已成为医疗机构的主要威胁。本研究描述了使用主动监测成功控制由产 NDM-1 的肺炎克雷伯菌 ST307 引起的医院暴发。暴发始于一名患者从当地医院转院。在我们医院 48 小时后,气管吸出物中发现一株耐美罗培南和产碳青霉烯酶的肺炎克雷伯菌。所有在重症监护病房(ICU)和神经科病房的患者均采取接触预防措施。对医院表面和设备、医护人员以及来自这些病房的患者进行了培养筛查。将粪便拭子放入肉汤中,然后进行 blaKPC、blaOXA-48、blaIMP、blaVIM 和 blaNDM 的 PCR,12 小时后直接从肉汤中进行 PCR。还对从肉汤中分离的产碳青霉烯酶种的 DNA 进行了 blaNDM-1 的 PCR。五天和九天后,又有两名患者的直肠拭子检测呈阳性。分子检测鉴定出 K. pneumoniae blaNDM-1 位于一个 130-kb 可接合质粒(IncY、IncFIIs 和 IncFIIY)上,ST307。在这三例患者出院后,监测仍在继续,三周后结果均为阴性,停止直肠拭子检查。总之,通过流行病学和微生物学监测,有可能控制由产 NDM-1 的肺炎克雷伯菌 ST307 引起的医院暴发。使用所采用的方法,在获得粪便样本后大约 15 小时即可获得粪便样本中 NDM 型基因的检测结果。