Yu Zanzhe, Lambie Mark, Chess James, Williams Andrew, Do Jun-Young, Topley Nicholas, Davies Simon J
Renji Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai, China.
Institute of Applied Clinical Science, Keele University, Stoke-on-Trent, United Kingdom.
Front Physiol. 2019 Feb 18;10:105. doi: 10.3389/fphys.2019.00105. eCollection 2019.
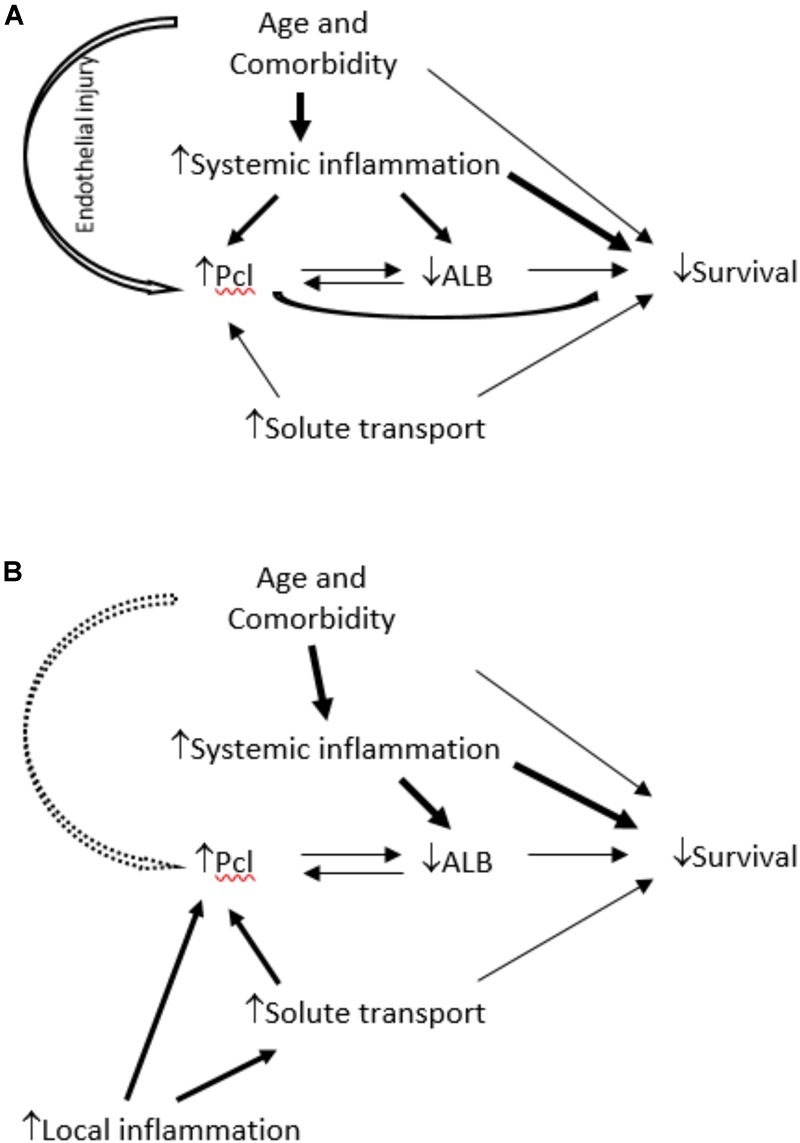
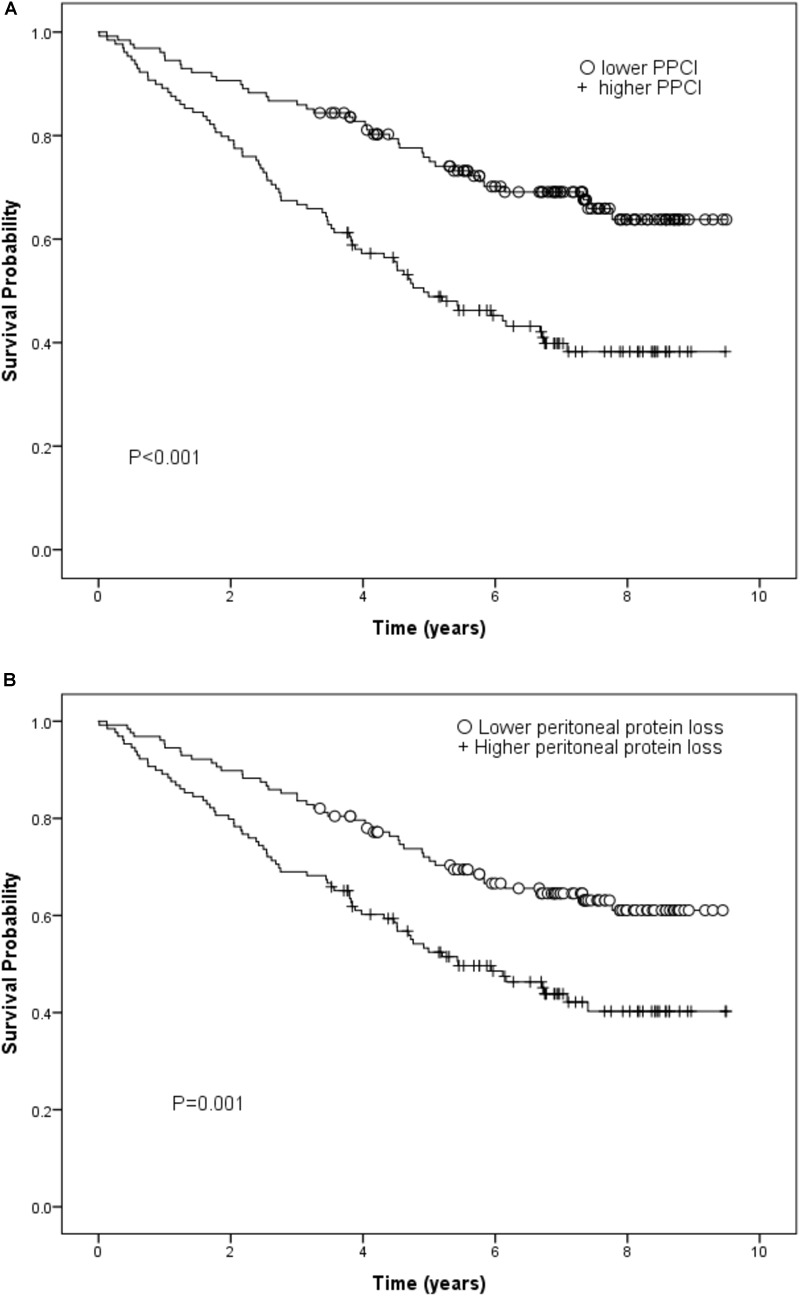
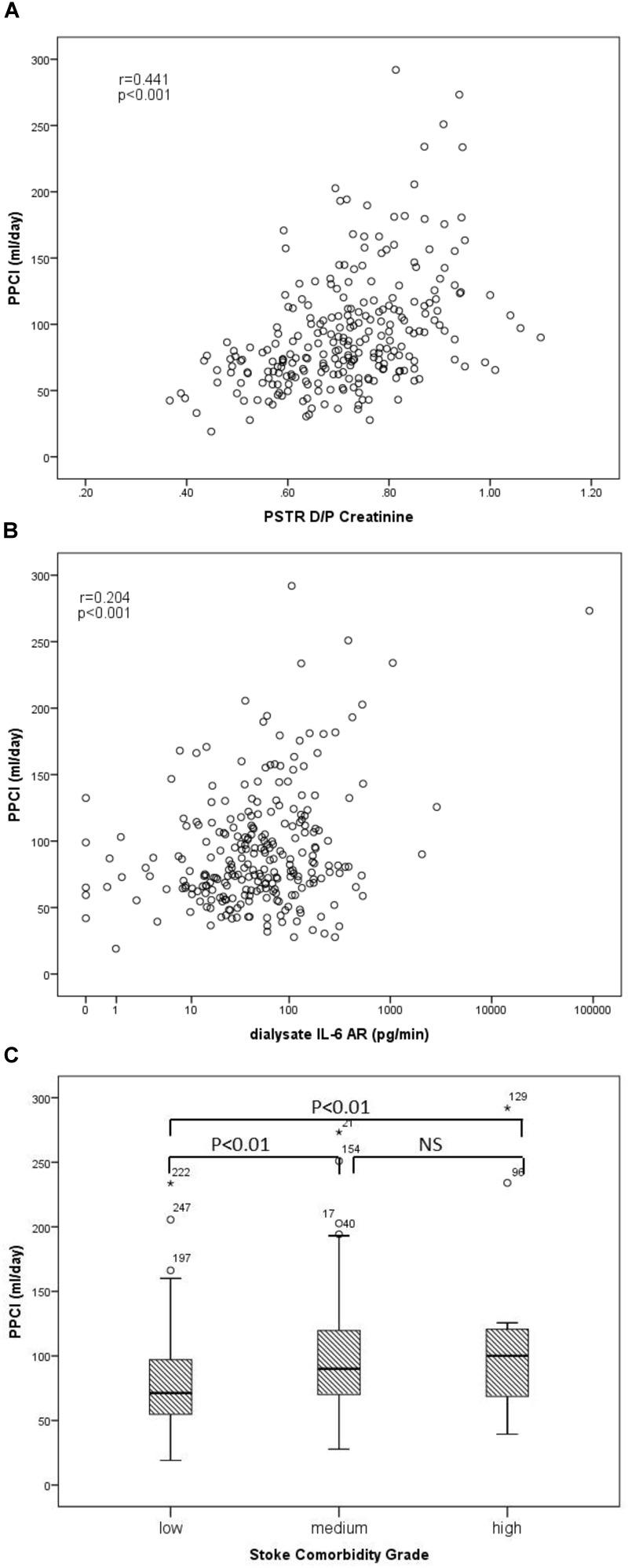
It is not clear whether the association of increased peritoneal protein clearance (PPCl) with worse survival on peritoneal dialysis (PD) is a consequence of either local or systemic inflammation or indicative of generalized endothelial dysfunction associated with comorbidity. To investigate this we determined the relationship of PPCl to comorbidity, membrane area (equivalent to low molecular weight peritoneal solute transport rate), local and systemic inflammation and hypoalbuminaemia, and for each of these with patient survival. 257 incident patients from three GLOBAL Fluid Study centers were included in this analysis. Clinical profiles were collected at baseline along with a peritoneal equilibration test, 24-h dialysate protein and paired plasma and dialysate cytokine measurements. Although peritoneal protein clearance was associated with increased age and severe comorbidity on univariate analysis, only dialysate IL-6, peritoneal solute transport rate, plasma albumin and cardiac comorbidities (ischaemic heart disease and left ventricular dysfunction) were independent explanatory variables on multivariate analysis. While peritoneal protein clearance and daily peritoneal protein loss were associated with survival in univariate analysis, on multivariate analysis only plasma IL-6, age, residual kidney function, comorbidity, and plasma albumin were independent predictors. Peritoneal protein clearance is primarily a function of peritoneal membrane area and local membrane inflammation. The association with comorbidity and survival is predominantly explained by its inverse relationship to hypoalbuminaemia, especially in diabetics.
腹膜透析(PD)时腹膜蛋白清除率(PPCl)增加与较差的生存率之间的关联,究竟是局部或全身炎症的结果,还是与合并症相关的全身性内皮功能障碍的表现,目前尚不清楚。为了研究这一问题,我们确定了PPCl与合并症、膜面积(等同于低分子量腹膜溶质转运率)、局部和全身炎症以及低白蛋白血症之间的关系,并分别研究了这些因素与患者生存率的关系。本分析纳入了来自全球液体研究中心三个研究点的257例新发病例。在基线时收集临床资料,同时进行腹膜平衡试验、24小时透析液蛋白以及配对的血浆和透析液细胞因子测量。单因素分析显示腹膜蛋白清除率与年龄增加和严重合并症相关,但多因素分析中只有透析液IL-6、腹膜溶质转运率、血浆白蛋白和心脏合并症(缺血性心脏病和左心室功能障碍)是独立的解释变量。单因素分析中腹膜蛋白清除率和每日腹膜蛋白丢失与生存率相关,但多因素分析中只有血浆IL-6、年龄、残余肾功能、合并症和血浆白蛋白是独立的预测因素。腹膜蛋白清除率主要取决于腹膜面积和局部膜炎症。与合并症和生存率的关联主要由其与低白蛋白血症的负相关来解释,尤其是在糖尿病患者中。