Rijal Komal Raj, Adhikari Bipin, Adhikari Nabaraj, Dumre Shyam Prakash, Banjara Mayur Sharma, Shrestha Upendra Thapa, Banjara Megha Raj, Singh Nihal, Ortegea Leonard, Lal Bibek Kumar, Thakur Garib Das, Ghimire Prakash
1Central Department of Microbiology, Tribhuvan University, Kirtipur, Kathmandu, Nepal.
2Centre for Tropical Medicine and Global Health, Nuffield Department of Medicine, University of Oxford, Oxford, UK.
Trop Med Health. 2019 Mar 27;47:21. doi: 10.1186/s41182-019-0148-7. eCollection 2019.
A significant reduction in malaria cases over the recent years in Nepal has encouraged the government to adopt a goal of "malaria-free nation by 2025." Nevertheless, to achieve this goal, it is critical to identify the epidemiological burden of malaria by specific regions and areas for an effective targeted intervention. The main objective of this study was to estimate the risk of malaria at Village Development Committee (VDC) level in Nepal based on disease, vector, parasite, and geography.
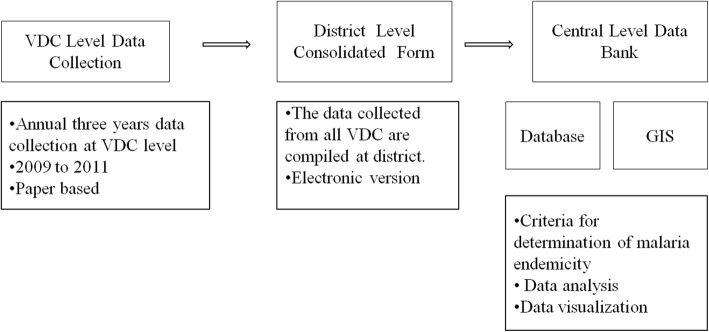
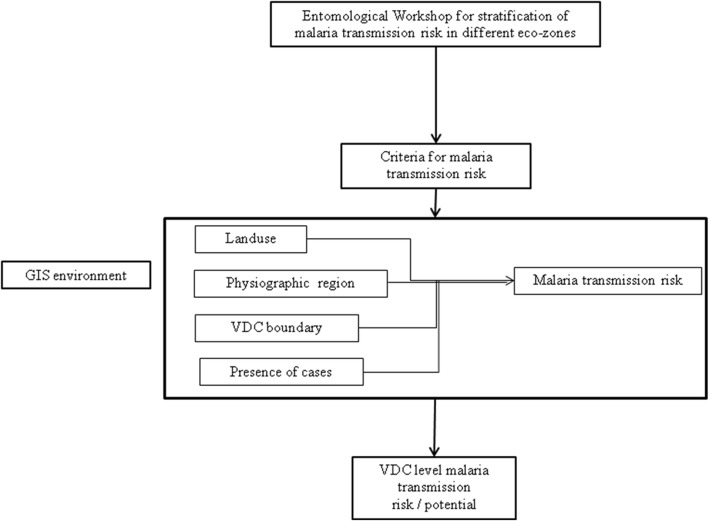
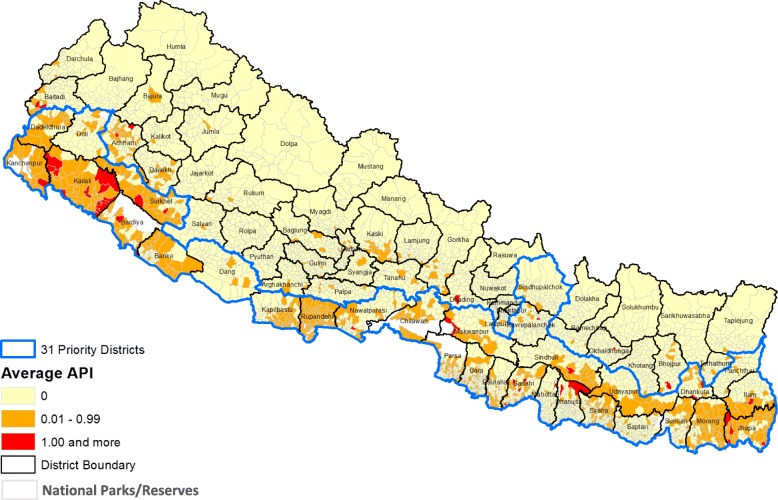
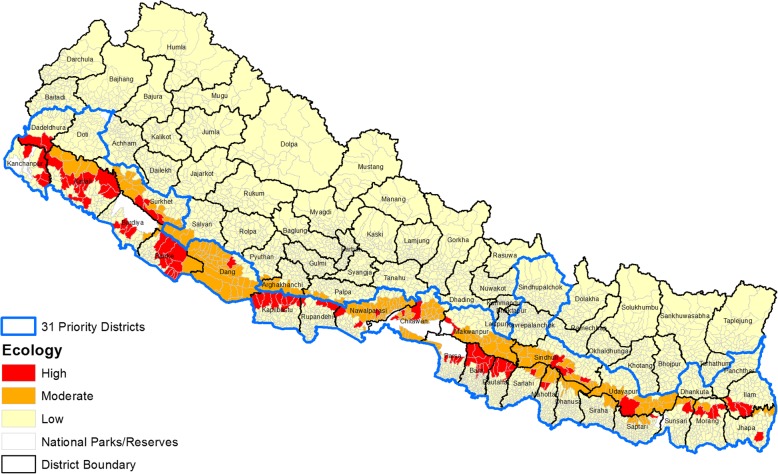
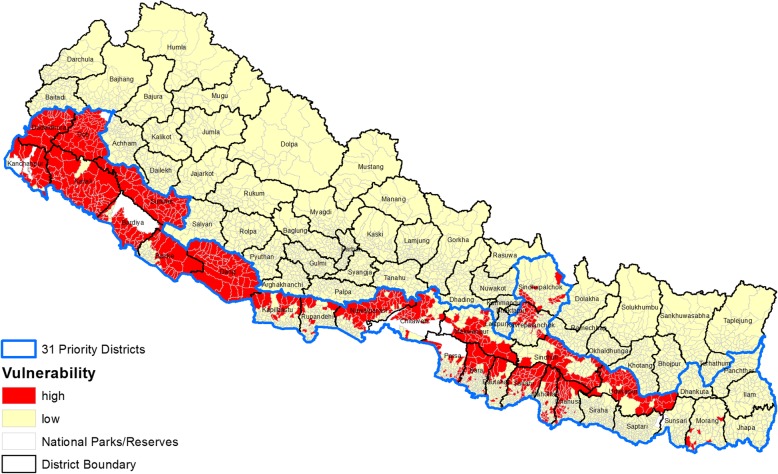
In 2012, the micro-stratification of malaria risk was carried out in 75 districts of Nepal. Instruments such as a questionnaire, case record forms, and guidelines for malaria micro-stratification were developed and pre-tested for necessary adaptations. Village Development Committee (VDC)-wise malaria data were analyzed using exploratory statistics and were stratified by geographical variables that contributed to the risk of malaria. To understand the transmission risk at VDC level, overlay analysis was done using ArcGIS 10. To ensure transparent, reproducible, and comprehensible risk assessment, standard scoring method was selected and utilized for data from 2009 to 2011. Thus identified, three major variables (key determinants) were given weights (wt.) accordingly to stratification of the malaria risk (disease burden, "0.3" wt.; ecology/vector transmission, "0.5" wt.; and vulnerability-population movement, "0.2" wt.). Malaria risk in a VDC was determined based on the overall scores and classified into four categories: no risk, low risk, moderate risk, and high risk.
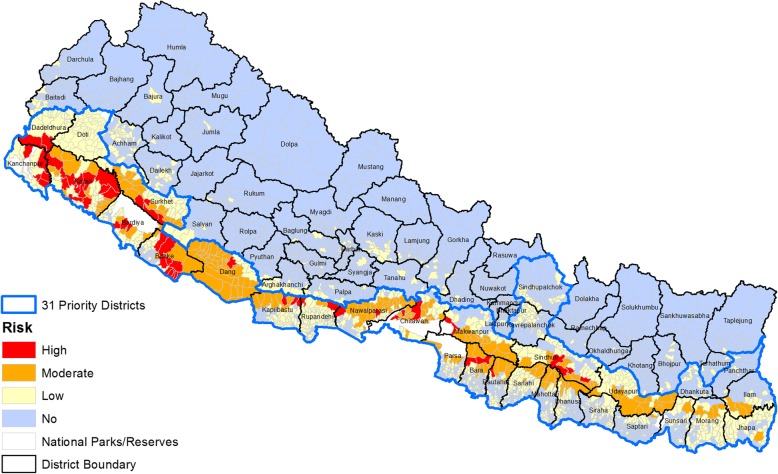
Analyzing the overall risk based on scoring of the total VDCs ( = 3976), 54 (1.36%), 201 (5.06%), 999 (25.13%), and 2718 (68.36%) were identified as high-, moderate-, low-, and no-risk categories for malaria, respectively. Based on the population statistics, 3.62%, 9.79%, 34.52%, and 52.05% of the country's total population live in high-risk, moderate-risk, low-risk, and no-risk VDCs for malaria, respectively. Our micro-stratification study estimates are 100,000 population at high risk. Regional distribution showed that the majority of the high-risk VDCs were identified in the Far- and Mid-western regions (19 and 18 VDCs) followed by Central and Western regions (10 and 7 VDCs) with no high-risk VDCs in the Eastern region. Similarly, 77, 59, 27, 24, and 14 VDCs of the Central, Mid-western, Western, Eastern, and Far-western regions, respectively, were found under moderate malaria risk. Of the low-risk VDCs, 353, 215, 191, 148, and 92 were respectively from the Central, Eastern, Western, Far-western, and Mid-western regions.
The current micro-stratification study provides insights on malaria risk up to the VDC level. This will help the malaria elimination program to target interventions at the local level thereby ensuring the best utilization of available resources to substantially narrowed-down target areas. With further updates and refinement, the micro-stratification approach can be employed to identify the risk areas up to smaller units within the VDCs (ward and villages).
近年来尼泊尔疟疾病例显著减少,这促使政府制定了“到2025年成为无疟疾国家”的目标。然而,要实现这一目标,通过特定地区和区域确定疟疾的流行病学负担以进行有效的针对性干预至关重要。本研究的主要目的是基于疾病、病媒、寄生虫和地理因素,估计尼泊尔乡村发展委员会(VDC)层面的疟疾风险。
2012年,在尼泊尔的75个区开展了疟疾风险的微观分层工作。开发了诸如问卷、病例记录表和疟疾微观分层指南等工具,并进行了预测试以作必要调整。利用探索性统计方法分析了按乡村发展委员会划分的疟疾数据,并按导致疟疾风险的地理变量进行分层。为了解乡村发展委员会层面的传播风险,使用ArcGIS 10进行了叠加分析。为确保风险评估透明、可重复且易于理解,选择并采用标准评分方法对2009年至2011年的数据进行分析。据此确定了三个主要变量(关键决定因素),并根据疟疾风险分层(疾病负担,权重“0.3”;生态/病媒传播,权重“0.5”;脆弱性 - 人口流动,权重“0.2”)相应地赋予权重。根据总分确定乡村发展委员会的疟疾风险,并分为四类:无风险、低风险、中度风险和高风险。
根据对所有乡村发展委员会(共3976个)的评分分析总体风险,分别有54个(1.36%)、201个(5.06%)、999个(25.13%)和2718个(68.36%)被确定为疟疾的高风险、中度风险、低风险和无风险类别。根据人口统计数据,该国总人口的3.62%、9.79%、34.52%和52.05%分别生活在疟疾高风险、中度风险、低风险和无风险的乡村发展委员会地区。我们的微观分层研究估计有10万人口处于高风险状态。区域分布显示,大多数高风险乡村发展委员会位于远西区和中西部地区(分别为19个和18个乡村发展委员会),其次是中部和西部地区(分别为10个和7个乡村发展委员会),东部地区没有高风险乡村发展委员会。同样,中部、中西部、西部、东部和远西部地区分别有77个、59个、27个、24个和14个乡村发展委员会处于中度疟疾风险。在低风险乡村发展委员会中,分别有353个、215个、191个、148个和92个来自中部、东部、西部、远西部和中西部地区。
当前的微观分层研究提供了直至乡村发展委员会层面的疟疾风险见解。这将有助于疟疾消除计划在地方层面进行针对性干预,从而确保最佳利用可用资源,大幅缩小目标区域。随着进一步更新和完善,微观分层方法可用于识别直至乡村发展委员会内更小单位(选区和村庄)的风险区域。