1 Swedish Institute for Disability Research, Department of Behavioural Sciences and Learning, Linköping University, Linköping, Sweden.
2 Rheumatology/Division of Neuro and Inflammation Sciences, Department of Clinical and Experimental Medicine, Linköping University, Linköping, Sweden.
Lupus. 2019 May;28(6):778-782. doi: 10.1177/0961203319846388. Epub 2019 May 2.
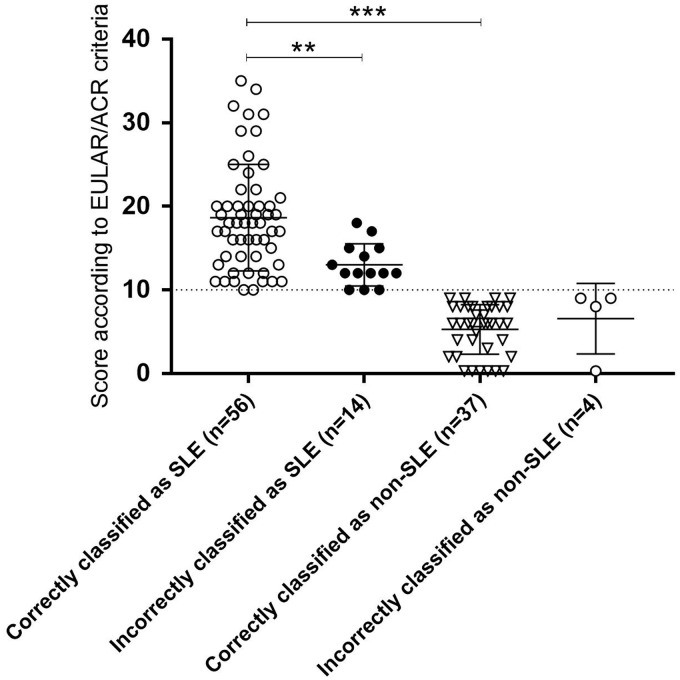
In a joint effort, the European League Against Rheumatism (EULAR) and the American College of Rheumatology (ACR) recently proposed new criteria for the classification of systemic lupus erythematosus (SLE) with the overarching goal to identify potential participants for clinical studies. Herein, we present the first independent evaluation of these criteria in comparison with older classification grounds using an adult Scandinavian study population of confirmed SLE cases and individuals with SLE-mimicking conditions. We included 56 confirmed SLE cases meeting the 1982 ACR criteria (ACR-82) and/or the Fries "diagnostic principle" (antinuclear antibodies on at least one occasion plus involvement of at least two defined organ systems) and 55 controls with possible systemic autoimmune disease, including the presence of any SLE-related autoantibody. The proposed EULAR/ACR criteria showed a diagnostic sensitivity of 93% (95% confidence interval (CI), 0.83-0.98) compared with 83% (95% CI, 0.72-0.91) for the updated ACR criteria from 1997. The diagnostic accuracy of all tested classification grounds was fairly similar, achieving approximately 85%. However, the disease specificity of the EULAR/ACR criteria reached only 73% (95% CI, 0.59-0.83), which was comparable with the 2012 Systemic Lupus International Collaborating Clinics (SLICC) criteria, 75% (95% CI, 0.61-0.85), but clearly lower than for ACR-82, 94% (95% CI, 0.83-0.99). In this first independent evaluation of a limited number of cases, we found comparable results with respect to diagnostic sensitivity, specificity and accuracy regarding the SLICC-12 and the proposed EULAR/ACR classification criteria. However, their specificity for SLE appeared to be lower compared with ACR-82.
在一项联合努力中,欧洲抗风湿病联盟(EULAR)和美国风湿病学会(ACR)最近提出了系统性红斑狼疮(SLE)的新分类标准,其首要目标是确定潜在的临床研究参与者。在此,我们使用经确认的 SLE 病例和具有 SLE 样表现的个体的斯堪的纳维亚成人研究人群,首次对这些标准进行了与旧分类标准的独立评估。我们纳入了 56 例符合 1982 年 ACR 标准(ACR-82)和/或 Fries“诊断原则”(至少一次出现抗核抗体加上至少两个定义的器官系统受累)的确诊 SLE 病例,以及 55 例可能患有系统性自身免疫性疾病的对照者,包括存在任何与 SLE 相关的自身抗体。与 1997 年更新的 ACR 标准相比,提出的 EULAR/ACR 标准显示出 93%(95%置信区间[CI],0.83-0.98)的诊断敏感性,而更新的 ACR 标准的诊断敏感性为 83%(95%CI,0.72-0.91)。所有测试分类标准的诊断准确性相当相似,约为 85%。然而,EULAR/ACR 标准的疾病特异性仅为 73%(95%CI,0.59-0.83),与 2012 年系统性红斑狼疮国际协作临床(SLICC)标准的 75%(95%CI,0.61-0.85)相当,但明显低于 ACR-82 的 94%(95%CI,0.83-0.99)。在对有限数量病例的首次独立评估中,我们发现 SLICC-12 和提出的 EULAR/ACR 分类标准在诊断敏感性、特异性和准确性方面具有可比的结果。然而,它们对 SLE 的特异性似乎低于 ACR-82。