Fernández-Barat Laia, Motos Ana, Panigada Mauro, Álvarez-Lerma Francisco, Viña Lucía, Lopez-Aladid Ruben, Ceccato Adrian, Bassi Gianluigi Li, Nicolau David P, Lopez Yuli, Muñoz Laura, Guerrero Laura, Soy Dolors, Israel Trinidad, Castro Pedro, Torres Antoni
Cellex Laboratory, CibeRes ((Centro de Investigación Biomédica en Red de Enfermedades Respiratorias, 06/06/0028), Institut d'Investigacions Biomèdiques August Pi i Sunyer (IDIBAPS), School of Medicine, University of Barcelona, C/ Casanova 143, 08036, Cellex laboratory, Barcelona, Spain.
Respiratory Intensive Care Unit Pneumology Department, Hospital Clínic, Barcelona, Spain.
Crit Care. 2019 Jul 10;23(1):251. doi: 10.1186/s13054-019-2523-5.
To compare the efficacy of systemic treatment with linezolid (LNZ) versus vancomycin (VAN) on methicillin-resistant Staphylococcus aureus (MRSA) burden and eradication in endotracheal tube (ETT) biofilm and ETT cuff from orotracheally intubated patients with MRSA respiratory infection.
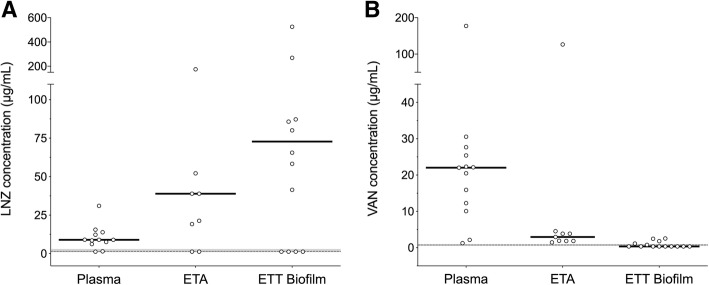
Prospective observational clinical study was carried out at four European tertiary hospitals. Plasma and endotracheal aspirate (ETA) levels of LNZ and VAN were determined 72 h after treatment initiation through high-performance liquid chromatography or bioassay. LNZ or VAN concentration in the ETT biofilm and MRSA burden and eradication was determined upon extubation. The minimum inhibitory concentration (MIC) for LNZ and VAN was assessed by E-test strips (Biomerieux®). Scanning electron microscopy images were obtained, and ETT biofilm thickness was compared between groups.
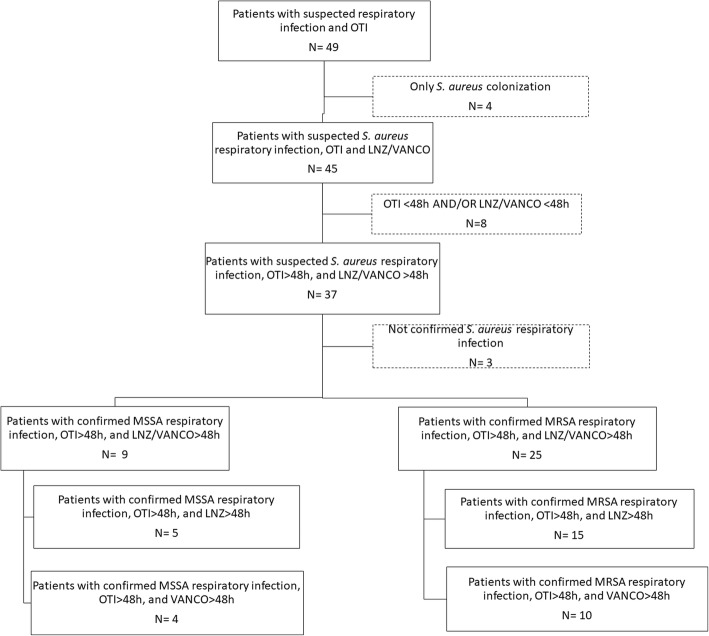
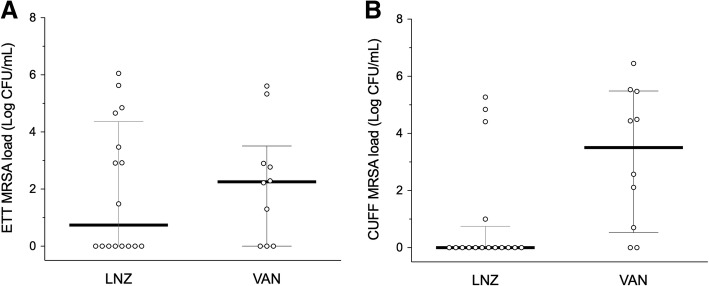
Twenty-five patients, 15 treated with LNZ and 10 with VAN, were included in the study. LNZ presented a significantly higher concentration (μg/mL) than VAN in ETT biofilm (72.8 [1.3-127.1] vs 0.4 [0.4-1.3], p < 0.001), although both drugs achieved therapeutic plasma levels 72 h after treatment initiation. Systemic treatment with LNZ achieved lower ETT cuff MRSA burdens than systemic treatment with VAN. Indeed, LNZ increased the MRSA eradication rate in ETT cuff compared with VAN (LNZ 75%, VAN 20%, p = 0.031).
In ICU patients with MRSA respiratory infection intubated for long periods, systemic treatment with LNZ obtains a greater beneficial effect than VAN in limiting MRSA burden in ETT cuff.
比较利奈唑胺(LNZ)与万古霉素(VAN)全身治疗对耐甲氧西林金黄色葡萄球菌(MRSA)负荷的影响,以及对经口气管插管的MRSA呼吸道感染患者气管内导管(ETT)生物膜和ETT套囊内MRSA的清除效果。
在四家欧洲三级医院进行前瞻性观察性临床研究。治疗开始72小时后,通过高效液相色谱法或生物测定法测定血浆和气管内吸出物(ETA)中LNZ和VAN的水平。拔管时测定ETT生物膜中LNZ或VAN的浓度、MRSA负荷及清除情况。通过E-test试纸(Biomerieux®)评估LNZ和VAN的最低抑菌浓度(MIC)。获取扫描电子显微镜图像,并比较各组间ETT生物膜厚度。
本研究纳入25例患者,其中15例接受LNZ治疗,10例接受VAN治疗。尽管两种药物在治疗开始72小时后均达到治疗性血浆水平,但ETT生物膜中LNZ的浓度(μg/mL)显著高于VAN(72.8 [1.3 - 127.1] 对比 0.4 [0.4 - 1.3],p < 0.001)。与VAN全身治疗相比,LNZ全身治疗使ETT套囊内MRSA负荷更低。实际上,与VAN相比,LNZ提高了ETT套囊内MRSA清除率(LNZ为75%,VAN为20%,p = 0.031)。
在长期插管的MRSA呼吸道感染重症监护病房患者中,LNZ全身治疗在限制ETT套囊内MRSA负荷方面比VAN具有更大的有益效果。