Department of Public Health, Amsterdam UMC, Amsterdam Public Health (APH) Research Institute, University of Amsterdam, Amsterdam, The Netherlands.
Department of Clinical Epidemiology, Biostatistics and Bioinformatics, Amsterdam UMC, University of Amsterdam, Amsterdam, The Netherlands.
Eur J Public Health. 2019 Aug 1;29(4):687-693. doi: 10.1093/eurpub/ckz012.
The burden of multimorbidity is likely higher in ethnic minority populations, as most individual diseases are more prevalent in minority groups. However, information is scarce. We examined ethnic inequalities in multimorbidity, and investigated to what extent they reflect differences in socioeconomic status (SES).
We included Healthy Life in an Urban Setting study participants of Dutch (N = 4582), South-Asian Surinamese (N = 3258), African Surinamese (N = 4267), Ghanaian (N = 2282), Turkish (N = 3879) and Moroccan (N = 4094) origin (aged 18-70 years). Educational level, employment status, income situation and multimorbidity were defined based on questionnaires. We described the prevalence and examined age-adjusted ethnic inequalities in multimorbidity with logistic regression analyses. To assess the contribution of SES, we added SES indicators to the age-adjusted model.
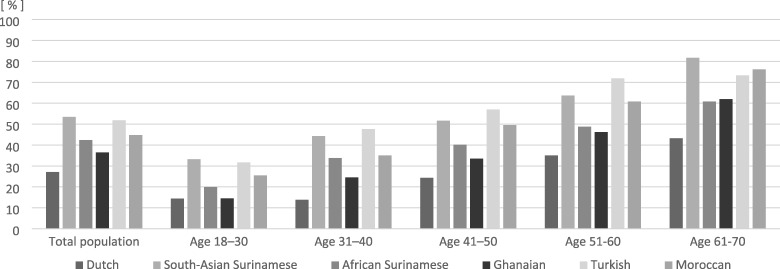
The prevalence of multimorbidity ranged from 27.1 to 53.4% in men and from 38.5 to 69.6% in women. The prevalence of multimorbidity in most ethnic minority groups was comparable to the prevalence among Dutch participants who were 1-3 decades older. After adjustment for SES, the odds of multimorbidity remained significantly higher in ethnic minority groups. For instance, age-adjusted OR for multimorbidity for the Turkish compared to the Dutch changed from 4.43 (3.84-5.13) to 2.34 (1.99-2.75) in men and from 5.35 (4.69-6.10) to 2.94 (2.54-3.41) in women after simultaneous adjustment for all SES indicators.
We found a significantly higher prevalence of multimorbidity in ethnic minority men and women compared to Dutch, and results pointed to an earlier onset of multimorbidity in ethnic minority groups. These inequalities in multimorbidity were not fully accounted for by differences in SES.
少数民族群体的多种疾病负担可能更高,因为大多数单病种在少数群体中更为普遍。然而,相关信息却很匮乏。我们研究了多种疾病在少数民族中的不平等现象,并探讨了这些差异在多大程度上反映了社会经济地位(SES)的差异。
我们纳入了荷兰(N=4582)、南亚苏里南(N=3258)、非洲苏里南(N=4267)、加纳(N=2282)、土耳其(N=3879)和摩洛哥(N=4094)裔的健康生活在城市环境研究参与者(年龄在 18-70 岁之间)。教育水平、就业状况、收入状况和多种疾病均根据问卷调查进行定义。我们描述了多种疾病的流行情况,并通过逻辑回归分析检查了年龄调整后的多种疾病的种族不平等现象。为了评估 SES 的贡献,我们将 SES 指标添加到年龄调整后的模型中。
男性的多种疾病患病率在 27.1%至 53.4%之间,女性的患病率在 38.5%至 69.6%之间。在大多数少数民族群体中,多种疾病的患病率与年龄相差 1-3 个十年的荷兰参与者的患病率相当。在调整 SES 后,少数民族群体发生多种疾病的几率仍然明显更高。例如,与荷兰相比,土耳其男性的多种疾病调整年龄后的优势比从 4.43(3.84-5.13)变为 2.34(1.99-2.75),女性从 5.35(4.69-6.10)变为 2.94(2.54-3.41),在同时调整所有 SES 指标后。
我们发现,与荷兰人相比,少数民族男性和女性的多种疾病患病率明显更高,并且结果表明少数民族群体的多种疾病发病年龄更早。这些多种疾病的不平等现象不能完全用 SES 差异来解释。