International Institute for Population Sciences, Govandi Station Road, Deonar, Mumbai, Maharashtra, 400088, India.
Department of Fertility Studies, International Institute for Population Sciences, Govandi Station Road, Deonar, Mumbai, 400088, India.
BMC Public Health. 2019 Jul 30;19(1):1020. doi: 10.1186/s12889-019-7342-8.
Rising health spending is associated with high out-of-pocket expenditure (OOPE), catastrophic health spending (CHS), increasing poverty, and impoverishment. Though studies have examined poverty and impoverishment effect of health spending in India, there is limited research on the regional patterns of health spending by type of health centers. This paper tests the hypothesis that the poor people from the poorer states of India pay significantly more for hospitalization in public health centers than those in the richer states of India.
Data from the Social Consumption of Health Survey (71st round, 2014), carried out by the National Sample Survey (NSS) is used in the analyses. Descriptive statistics, log-linear regression model and tobit model were used to examine the determinants and variations in health spending.
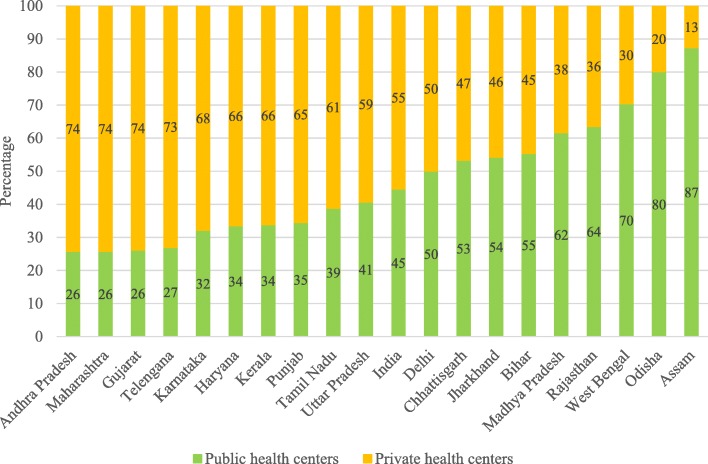
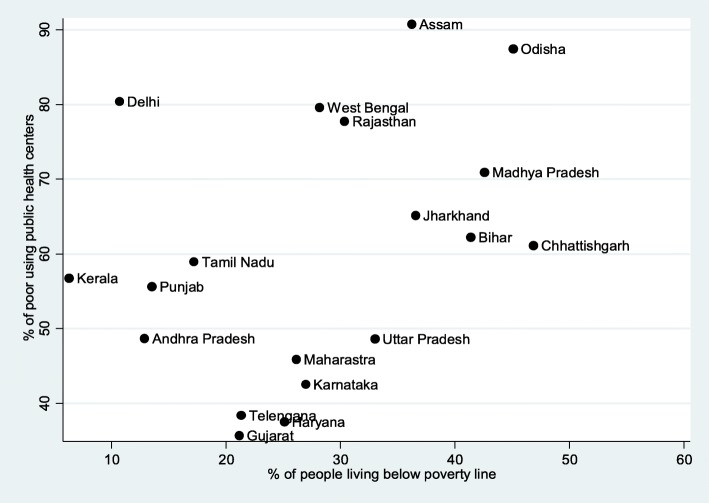
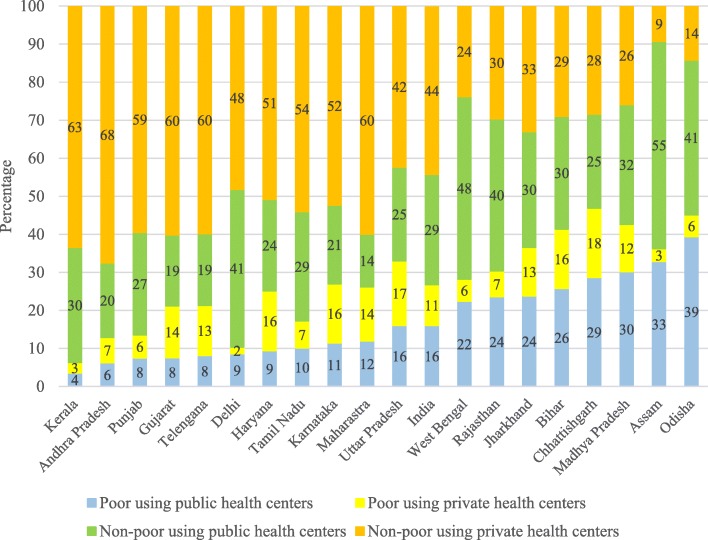
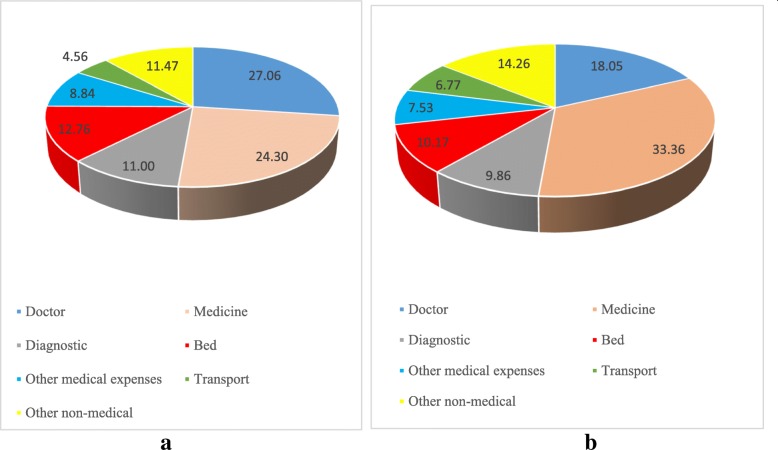
Inter-state variations in the utilization of public health services and the OOPE on hospitalization are high in India. States with high levels of poverty make higher use of the public health centers and yet incur high OOPE. In 2014, the mean OOPE per episode of hospitalization in public health centers in India was ₹5688 and ₹4264 for the economically poor households. It was lowest in the economically developed state of Tamil Nadu and highest in the economically poorer state of Bihar. The OOPE per episode of hospitalization in public health centers among the poor in the poorer states was at least twice that in Tamil Nadu. Among the poor using public health centers, the share of direct cost account 24% in Tamil Nadu compared to over 80% in Bihar, Odisha and other poorer states. Adjusting for socio-economic correlates, the cost of hospitalization per episode (CHPE) among the poor using public health centers was 51% lower than for the non-poor using private health centers in India.
The poor people in the poorer states in India pay significantly more to avail hospitalization in public health centers than those in the developed states. Provision of free medicines, surgery and free diagnostic tests in public health centers may reduce the high OOPE and medical poverty in India.
医疗支出的增加与自费支出(OOPE)、灾难性医疗支出(CHS)、贫困和贫困加剧有关。尽管已有研究考察了印度医疗支出对贫困和贫困的影响,但关于按卫生中心类型划分的卫生支出区域模式的研究有限。本文检验了这样一个假设,即来自印度较贫困邦的贫困人口在公立卫生中心住院治疗时支付的费用明显高于来自印度较富裕邦的贫困人口。
本研究使用了全国抽样调查(NSS)进行的社会卫生消费调查(第 71 轮,2014 年)的数据。采用描述性统计、对数线性回归模型和 Tobit 模型来检验卫生支出的决定因素和变化。
印度各邦之间公共卫生服务的利用和住院治疗的自费支出存在较大差异。贫困程度较高的邦更倾向于利用公立卫生中心,但自费支出也较高。2014 年,印度公立卫生中心每次住院治疗的自费支出平均值为 5688 卢比,经济贫困家庭为 4264 卢比。经济发达的泰米尔纳德邦最低,经济欠发达的比哈尔邦最高。较贫困邦的贫困人口在公立卫生中心每次住院治疗的自费支出至少是泰米尔纳德邦的两倍。在使用公立卫生中心的贫困人口中,直接费用占比在泰米尔纳德邦为 24%,而在比哈尔邦、奥里萨邦和其他较贫困邦则超过 80%。在调整了社会经济相关因素后,印度使用公立卫生中心的贫困人口每次住院治疗的费用(CHPE)比使用私立卫生中心的非贫困人口低 51%。
与发达邦的贫困人口相比,来自印度较贫困邦的贫困人口在公立卫生中心住院治疗时支付的费用要高得多。在公立卫生中心提供免费药品、手术和免费诊断检查可能会降低印度的自费支出和医疗贫困。