Centre for Medical and Health Sciences Education (CMHSE), University of Auckland, Auckland City Hospital, Building 599, level 12.025, 2 Park Rd. Grafton, Auckland, 1142, New Zealand.
BMC Med Educ. 2019 Aug 13;19(1):306. doi: 10.1186/s12909-019-1746-0.
Regulatory authorities in healthcare are authorised to develop and assess the cultural competence of their professionals. There remains significant diversity on approaches to cultural competency training and assessment. Little evidence exists about whether existing cultural competency training leads to improved patient health outcomes and reductions in health disparity.
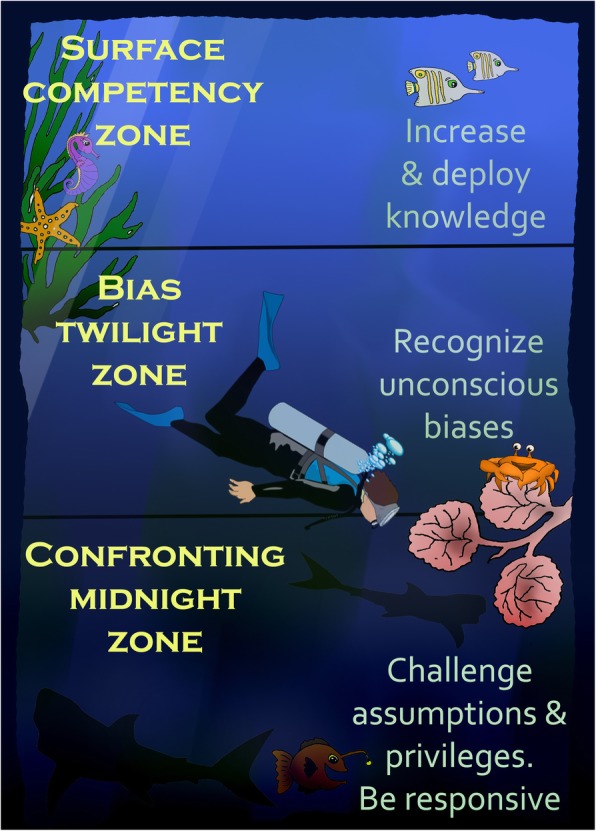
In this paper I frame cultural competency as analogous to the ocean and consisting of three zones: surface competency zone, bias twilight zone, and the confronting midnight zone. The surface competency zone focuses on deployment of culturally-specific knowledge: what people see, say, and do. The bias twilight zone is where people engage in critical reflection on their inherent/unconscious biases, and how such biases inform their thoughts and practices. The confronting midnight zone is where people engage in critical consciousness and self-awareness. Here they look beyond their biases to interrogate their power and positionality in society (their own privileges and centralisation). This attention is coupled with a commitment to social justice and to working within their means to reduce health disparities.
I suggest surface cultural competency is somewhat easier to see, teach and reach than the bias twilight or confronting midnight zones. But it is these deeper zones that cultural competency training needs to attend to if we are to see systemic cultural changes in healthcare provision. Research assessing the extent by which cultural competency training within each zone informs improved patient outcomes and reductions in health disparity is called for.
医疗保健监管机构被授权开发和评估其专业人员的文化能力。在文化能力培训和评估方法上仍然存在很大的多样性。关于现有的文化能力培训是否能改善患者的健康结果并减少健康差距,几乎没有证据。
在本文中,我将文化能力比作海洋,由三个区域组成:表面能力区、偏见黄昏区和直面午夜区。表面能力区侧重于运用特定文化的知识:人们看到、说和做的。偏见黄昏区是人们对内在/无意识偏见进行批判性反思的地方,以及这些偏见如何影响他们的思想和实践。直面午夜区是人们进行批判性意识和自我意识的地方。在这里,他们超越偏见,审视自己在社会中的权力和地位(自己的特权和中心化)。这种关注伴随着对社会正义的承诺,并致力于在自己的能力范围内努力减少健康差距。
我认为表面的文化能力比偏见黄昏区或直面午夜区更容易看到、教授和达到。但是,如果我们要看到医疗服务提供方面的系统性文化变革,文化能力培训需要关注这些更深层次的区域。需要进行研究,评估每个区域的文化能力培训在改善患者结果和减少健康差距方面的程度。