Kim Nicole J, Pearson Meredith, Vutien Philip, Su Feng, Moon Andrew M, Berry Kristin, Green Pamela K, Williams Emily C, Ioannou George N
Division of Gastroenterology University of Washington Seattle WA.
Division of Gastroenterology University of North Carolina Chapel Hill NC.
Hepatol Commun. 2020 Jan 2;4(2):314-324. doi: 10.1002/hep4.1464. eCollection 2020 Feb.
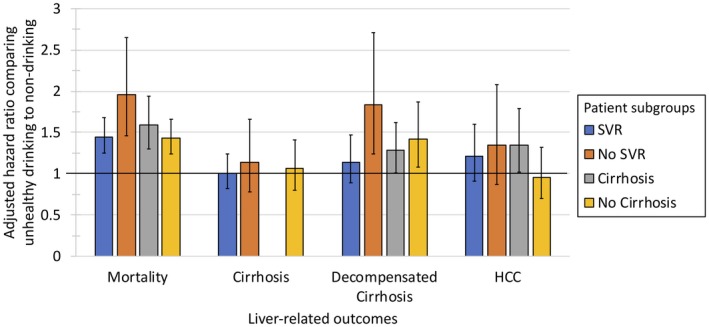
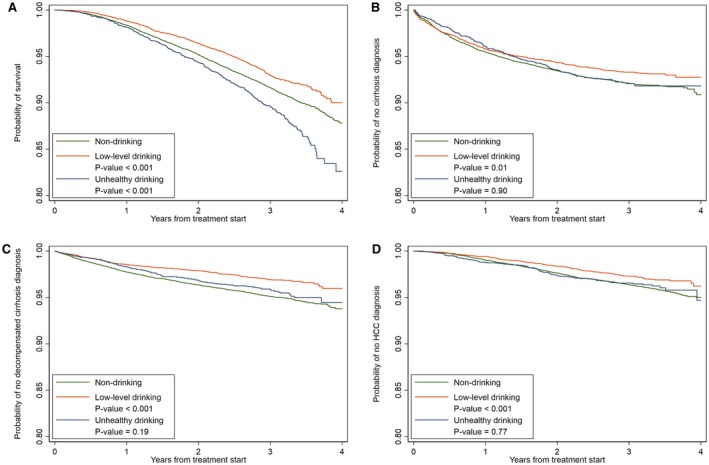
Outcomes related to alcohol use after hepatitis C virus (HCV) treatment are unknown in the direct-acting antiviral (DAA) era. We assessed levels of alcohol use before and after HCV treatment and their association with long-term outcomes in a cohort of U.S. veterans. In this retrospective cohort analysis, 29,037 patients who initiated DAA regimens between 2013 and 2015 were followed for a mean of 3.04 years. We categorized alcohol use into three categories (nondrinking, low-level drinking, and unhealthy drinking) using Alcohol Use Disorders Identification Test-Consumption questionnaires administered within 1 year before (baseline) and after treatment. Multivariable Cox proportional hazards regression was used to determine the associations between alcohol use and mortality or liver-related outcomes. Before DAA treatment, 68% of veterans reported nondrinking, 22.9% reported low-level drinking, and 9.1% reported unhealthy drinking. Compared to patients with baseline non-drinking, those with unhealthy drinking had a higher risk of mortality (adjusted hazard ratio [HR] 1.53, 95% confidence interval [CI]: 1.34-1.75) and decompensated cirrhosis (adjusted HR 1.30, 95% CI: 1.06-1.59) and lower likelihood of liver transplantation (adjusted HR 0.24, 95% CI: 0.06-0.92). These associations were greater in patients without sustained virologic response than in those with sustained virologic response. When alcohol use before and after treatment was modeled as a time-varying covariate, similar associations were observed. Survival analysis also found that unhealthy drinking was significantly associated with a lower probability of survival compared with nondrinking. Low-level alcohol use was not associated with increased risk of adverse outcomes. In this large cohort of U.S. veterans with HCV who received DAAs, unhealthy drinking was common and associated with a higher risk of posttreatment mortality. Interventions to achieve alcohol cessation before and during antiviral treatment should be encouraged.
在直接作用抗病毒药物(DAA)时代,丙型肝炎病毒(HCV)治疗后与酒精使用相关的结果尚不清楚。我们评估了美国退伍军人队列中HCV治疗前后的酒精使用水平及其与长期结果的关联。在这项回顾性队列分析中,对2013年至2015年间开始使用DAA方案的29,037名患者进行了平均3.04年的随访。我们使用在治疗前(基线)和治疗后1年内进行的酒精使用障碍识别测试-消费问卷,将酒精使用分为三类(不饮酒、低水平饮酒和不健康饮酒)。多变量Cox比例风险回归用于确定酒精使用与死亡率或肝脏相关结果之间的关联。在DAA治疗前,68%的退伍军人报告不饮酒,22.9%报告低水平饮酒,9.1%报告不健康饮酒。与基线不饮酒的患者相比,不健康饮酒的患者有更高的死亡风险(调整后的风险比[HR]为1.53,95%置信区间[CI]:1.34-1.75)和失代偿性肝硬化风险(调整后的HR为1.30,95%CI:1.06-1.59),以及更低的肝移植可能性(调整后的HR为0.24,95%CI:0.06-0.92)。这些关联在没有持续病毒学应答的患者中比在有持续病毒学应答的患者中更大。当将治疗前后的酒精使用作为时间变化协变量进行建模时,观察到了类似的关联。生存分析还发现,与不饮酒相比,不健康饮酒与较低的生存概率显著相关。低水平饮酒与不良结局风险增加无关。在这一接受DAA治疗的大量美国退伍军人HCV队列中,不健康饮酒很常见,且与治疗后更高的死亡风险相关。应鼓励在抗病毒治疗前和治疗期间采取干预措施以实现戒酒。