Dept of Applied Physics, University of Eastern Finland, Kuopio, Finland
Diagnostic Imaging Center, Kuopio University Hospital, Kuopio, Finland.
Eur Respir J. 2020 Apr 9;55(4). doi: 10.1183/13993003.01849-2019. Print 2020 Apr.
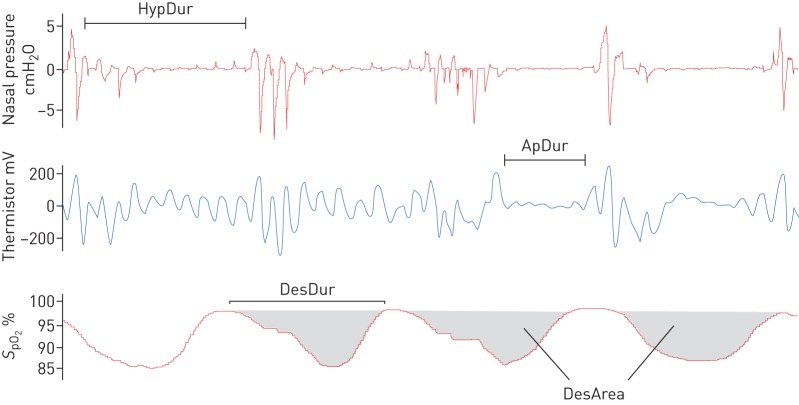
Current diagnostic parameters estimating obstructive sleep apnoea (OSA) severity have a poor connection to the psychomotor vigilance of OSA patients. Thus, we aimed to investigate how the severity of apnoeas, hypopnoeas and intermittent hypoxaemia is associated with impaired vigilance.We retrospectively examined type I polysomnography data and corresponding psychomotor vigilance tasks (PVTs) of 743 consecutive OSA patients (apnoea-hypopnoea index (AHI) ≥5 events·h). Conventional diagnostic parameters ( AHI and oxygen desaturation index (ODI)) and novel parameters ( desaturation severity and obstruction severity) incorporating duration of apnoeas and hypopnoeas as well as depth and duration of desaturations were assessed. Patients were grouped into quartiles based on PVT outcome variables. The odds of belonging to the worst-performing quartile were assessed. Analyses were performed for all PVT outcome variables using binomial logistic regression.A relative 10% increase in median depth of desaturations elevated the odds (OR 1.20-1.37, p<0.05) of prolonged mean and median reaction times as well as increased lapse count. Similarly, an increase in desaturation severity (OR 1.26-1.52, p<0.05) associated with prolonged median reaction time. Female sex (OR 2.21-6.02, p<0.01), Epworth Sleepiness Scale score (OR 1.05-1.07, p<0.01) and older age (OR 1.01-1.05, p<0.05) were significant risk factors in all analyses. In contrast, increases in conventional AHI, ODI and arousal index were not associated with deteriorated PVT performance.These results show that our novel parameters describing the severity of intermittent hypoxaemia are significantly associated with increased risk of impaired PVT performance, whereas conventional OSA severity and sleep fragmentation metrics are not. These results underline the importance of developing the assessment of OSA severity beyond the AHI.
目前用于评估阻塞性睡眠呼吸暂停(OSA)严重程度的诊断参数与 OSA 患者的精神警觉性相关性较差。因此,我们旨在研究呼吸暂停、低通气和间歇性低氧血症的严重程度与警觉性受损之间的关系。
我们回顾性地检查了 743 例连续 OSA 患者(呼吸暂停-低通气指数(AHI)≥5 次/小时)的 I 型多导睡眠图数据和相应的精神运动警觉任务(PVT)。评估了传统诊断参数(AHI 和氧减指数(ODI))和新参数(低氧严重程度和阻塞严重程度),包括呼吸暂停和低通气的持续时间以及低氧的深度和持续时间。根据 PVT 结果变量将患者分为四组。评估属于表现最差的四分之一的几率。使用二项逻辑回归分析所有 PVT 结果变量。
低氧深度中位数增加 10%,则平均和中位数反应时间延长以及漏答数增加的几率(OR 1.20-1.37,p<0.05)升高。同样,低氧严重程度增加(OR 1.26-1.52,p<0.05)与中位数反应时间延长相关。在所有分析中,女性(OR 2.21-6.02,p<0.01)、Epworth 嗜睡量表评分(OR 1.05-1.07,p<0.01)和年龄较大(OR 1.01-1.05,p<0.05)是显著的危险因素。相比之下,传统 AHI、ODI 和觉醒指数的增加与 PVT 性能恶化无关。
这些结果表明,我们描述间歇性低氧严重程度的新参数与 PVT 表现受损的风险增加显著相关,而传统的 OSA 严重程度和睡眠片段化指标则没有。这些结果强调了超越 AHI 评估 OSA 严重程度的重要性。