Tirore Mengistu Girma, Atey Tesfay Mehari, Mezgebe Haftay Berhane
1Department of Pharmacy, College of Health Sciences, Adigrat University, Adigrat, Tigray Ethiopia.
2Department of Clinical Pharmacy, School of Pharmacy, College of Health Sciences, Mekelle University, Mekelle, Tigray Ethiopia.
BMC Nutr. 2017 Jul 25;3:66. doi: 10.1186/s40795-017-0186-7. eCollection 2017.
Severe acute malnutrition remains the major cause of morbidity and mortality for children under five years of age in developing countries. The prevalence of wasting, underweight and stunting has remained high in Ethiopia and even unacceptably higher in Tigray region. The objective of the study is to assess the survival status and treatment outcome of patients with severe acute malnutrition and to identify contributing factors for poor treatment outcome.
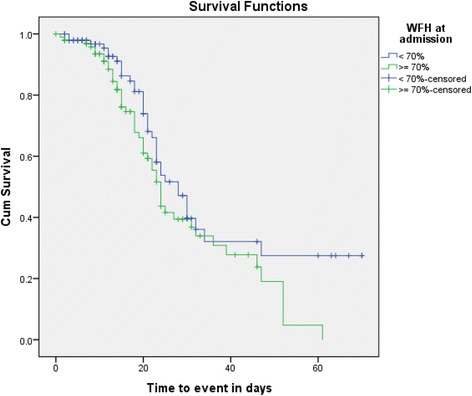
An institutional-based cross-sectional study was conducted on 195 patients, selected using systematic random sampling technique, from 24-Mar-2015 to 7-Jun-2015 in Ayder Referral Hospital. Logistic regression was carried out to identify factors associated with treatment outcome. Rates of mortality associated with the disease were determined using Kaplan-Meier survival analysis. A Log Rank, Breslow, and Tarone-Ware test were employed for the overall comparisons of the survival curves. Statistical significance was declared at - value <0.05.
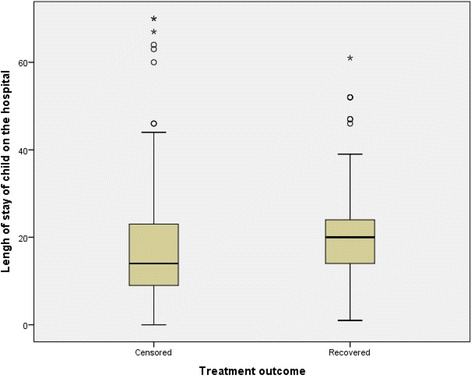
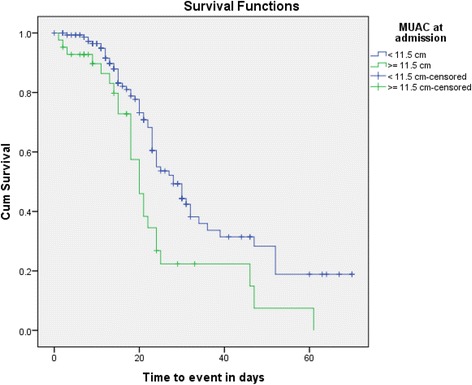
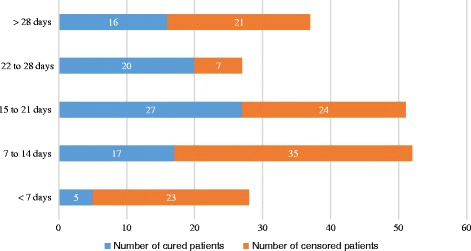
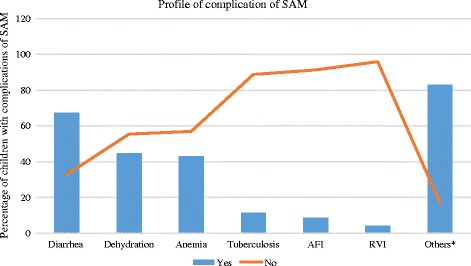
Out of 195 children admitted with SAM, the cure, death, defaulter, non-respondent and transferred-out rates were 22.1%, 3.6%, 43.6%, 9.2% and 21.5% respectively. Overall, 43.6% of the children were recovered from their disease. The mean length of stay of a 'recovered' child in the hospital was 21.56 ±1.27 days (95% CI: 19.04-24.09 days). Free from acute febrile illness (AOR = 4.20, 95% CI: 1.10-16.09, < 0.036) and usage of deworming medications (AOR = 0.36, 95% CI: 0.14-0.93, < 0.036) were significantly associated with positive and negative treatment outcomes respectively. Children with >70% of weight for height (WFH) and mid-upper arm circumference (MUAC) of >12 cm at admission had a better treatment outcome than children with WFH of ≤ 70% ( < 0.038) and MUAC of ≤ 12 cm ( < 0.090). Treatment using ready-to-used therapeutic food (RUTF) provided a longer all-cause mortality protection than the treatment using F-75 and F-100 ( < 0.010).
The cure rate in this study was found to be sub-optimal. Absence of acute febrile illness and deworming medication use were factors contributing to good treatment outcome. A WFH of >70%, MUAC of ≥ 12 cm and treatment using RUTF provided a longer all-cause mortality protection.
重度急性营养不良仍然是发展中国家五岁以下儿童发病和死亡的主要原因。在埃塞俄比亚,消瘦、体重不足和发育迟缓的患病率一直居高不下,在提格雷地区甚至高得令人无法接受。本研究的目的是评估重度急性营养不良患者的生存状况和治疗效果,并确定导致治疗效果不佳的因素。
2015年3月24日至2015年6月7日,在阿伊德转诊医院采用系统随机抽样技术,对195例患者进行了一项基于机构的横断面研究。进行逻辑回归以确定与治疗效果相关的因素。使用Kaplan-Meier生存分析确定与该疾病相关的死亡率。采用对数秩检验、Breslow检验和Tarone-Ware检验对生存曲线进行总体比较。当P值<0.05时,表明具有统计学意义。
在195例因重度急性营养不良入院的儿童中,治愈、死亡、失访、无反应和转出率分别为22.1%、3.6%、43.6%、9.2%和21.5%。总体而言,43.6%的儿童从疾病中康复。“康复”儿童在医院的平均住院时间为21.56±1.27天(95%CI:19.04 - 24.09天)。无急性发热性疾病(AOR = 4.20,95%CI:1.10 - 16.09,P < 0.036)和使用驱虫药物(AOR = 0.36,95%CI:0.14 - 0.93,P < 0.036)分别与积极和消极的治疗效果显著相关。入院时身高别体重(WFH)>70%且上臂中段周长(MUAC)>12 cm的儿童比WFH≤70%(P < 0.038)和MUAC≤12 cm(P < 0.090)的儿童治疗效果更好。使用即食治疗食品(RUTF)进行治疗比使用F - 75和F - 100进行治疗提供了更长时间的全因死亡率保护(P < 0.010)。
本研究中的治愈率不理想。无急性发热性疾病和使用驱虫药物是导致良好治疗效果的因素。WFH>70%、MUAC≥12 cm以及使用RUTF进行治疗提供了更长时间的全因死亡率保护。