Nuffield Department of Primary Care Health Sciences, University of Oxford, Oxford, UK.
Bodleian Health Care Libraries, University of Oxford, Oxford, UK.
BMC Med. 2020 Mar 13;18(1):49. doi: 10.1186/s12916-020-1510-7.
Social prescribing is a way of addressing the 'non-medical' needs (e.g. loneliness, debt, housing problems) that can affect people's health and well-being. Connector schemes (e.g. delivered by care navigators or link workers) have become a key component to social prescribing's delivery. Those in this role support patients by either (a) signposting them to relevant local assets (e.g. groups, organisations, charities, activities, events) or (b) taking time to assist them in identifying and prioritising their 'non-medical' needs and connecting them to relevant local assets. To understand how such connector schemes work, for whom, why and in what circumstances, we conducted a realist review.
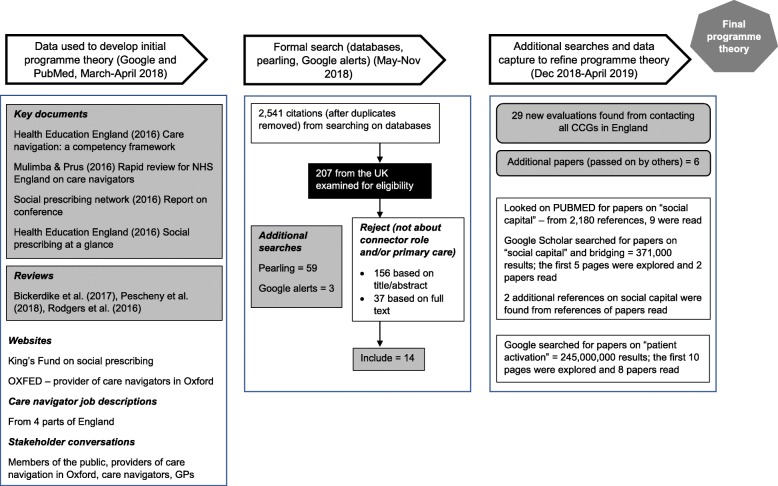
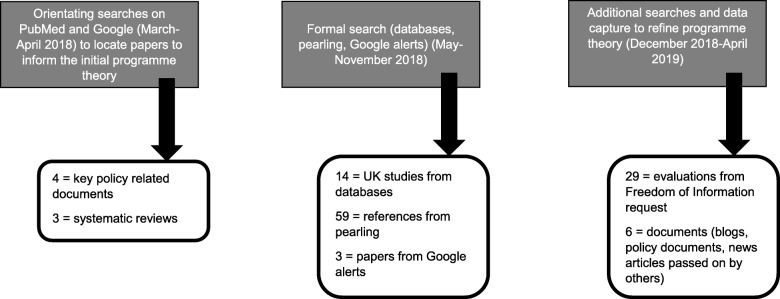
A search of electronic databases was supplemented with Google alerts and reference checking to locate grey literature. In addition, we sent a Freedom of Information request to all Clinical Commissioning Groups in England to identify any further evaluations of social prescribing connector schemes. Included studies were from the UK and focused on connector schemes for adult patients (18+ years) related to primary care.
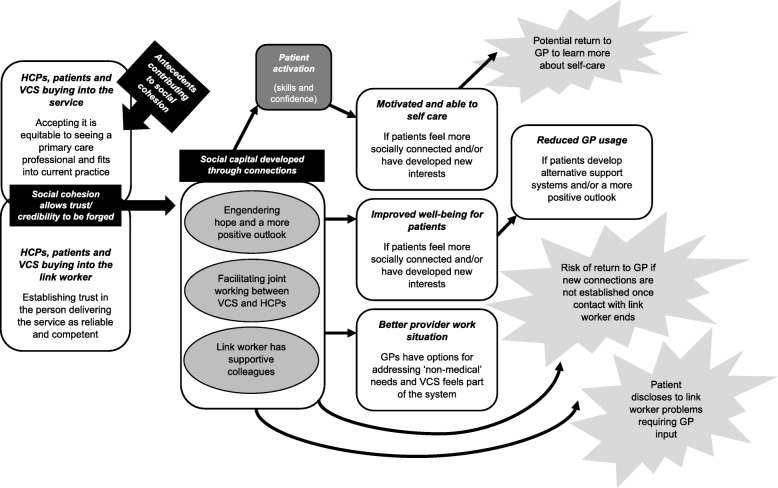
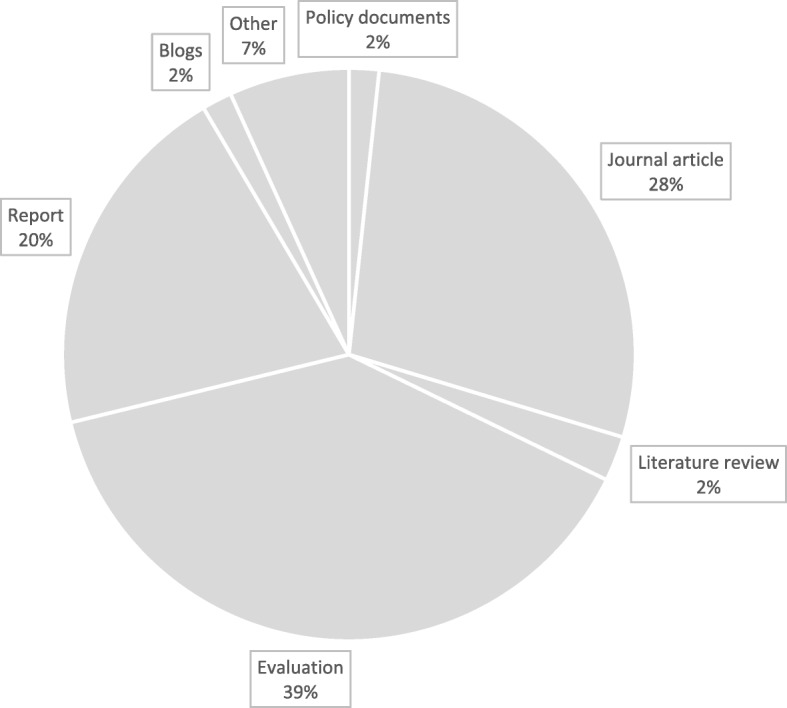
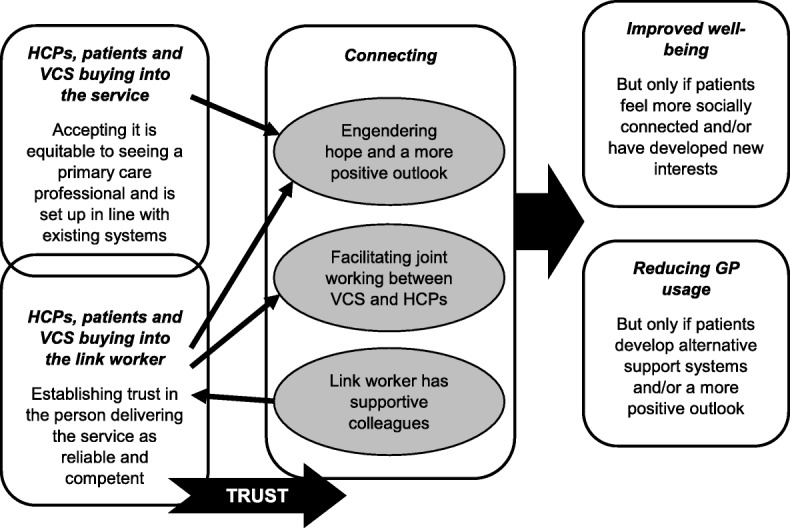
Our searches resulted in 118 included documents, from which data were extracted to produce context-mechanism-outcome configurations (CMOCs). These CMOCs underpinned our emerging programme theory that centred on the essential role of 'buy-in' and connections. This was refined further by turning to existing theories on (a) social capital and (b) patient activation.
Our realist review highlights how connector roles, especially link workers, represent a vehicle for accruing social capital (e.g. trust, sense of belonging, practical support). We propose that this then gives patients the confidence, motivation, connections, knowledge and skills to manage their own well-being, thereby reducing their reliance on GPs. We also emphasise within the programme theory situations that could result in unintended consequences (e.g. increased demand on GPs).
社会处方是一种解决可能影响人们健康和福祉的“非医疗”需求(例如孤独、债务、住房问题)的方法。连接器计划(例如由护理导航员或联络工作人员提供)已成为社会处方交付的关键组成部分。在这个角色中,他们通过以下两种方式来支持患者:(a) 将他们转介到相关的本地资源(例如团体、组织、慈善机构、活动、事件),或 (b) 花时间帮助他们确定和优先考虑他们的“非医疗”需求,并将他们与相关的本地资源联系起来。为了了解这种连接器计划是如何运作的、为谁服务、为什么以及在什么情况下运作,我们进行了一项实际主义审查。
对电子数据库进行了搜索,并通过 Google 警报和参考文献检查来查找灰色文献。此外,我们向英格兰的所有临床委托组发送了信息自由请求,以确定对社会处方连接器计划的任何进一步评估。纳入的研究来自英国,重点是与初级保健相关的成年患者(18 岁及以上)的连接器计划。
我们的搜索结果包括 118 份纳入的文件,从中提取数据以生成上下文-机制-结果配置(CMOC)。这些 CMOC 构成了我们新兴计划理论的基础,该理论集中在“认同”和联系的关键作用上。通过转向关于(a)社会资本和(b)患者激活的现有理论,这一理论得到了进一步的完善。
我们的实际主义审查强调了连接器角色(特别是联络工作人员)如何代表积累社会资本的工具(例如信任、归属感、实际支持)。我们提出,这使患者有信心、动力、联系、知识和技能来管理自己的健康,从而减少对全科医生的依赖。我们还在计划理论中强调了可能导致意外后果的情况(例如,对全科医生的需求增加)。