University College Dublin Centre for Interdisciplinary Research, Teaching and Innovation in Health Systems (UCD IRIS), School of Nursing, Midwifery & Health Systems, Health Sciences Centre, University College Dublin, Dublin 4, Ireland.
BMC Health Serv Res. 2020 Mar 30;20(1):261. doi: 10.1186/s12913-020-05129-1.
There is accumulating evidence for the value of collective and shared approaches to leadership. However, relatively little research has explored collective leadership in healthcare and thus, there is a lack understanding of the mechanisms that promote or inhibit the practice of collective leadership in healthcare teams. This study describes the development of an initial programme theory (IPT) to provide insight into the mechanisms underpinning the enactment of collective leadership.
This IPT was informed by a multiple-method data collection process. The first stage involved a realist synthesis of the literature on collective leadership interventions in healthcare settings (n = 21 studies). Next, we presented initial findings to receive feedback from a realist research peer support group. Interviews with members of teams identified as working collectively (n = 23) were then conducted and finally, we consulted with an expert panel (n = 5). Context-mechanism-outcome configurations (CMOCs) were extrapolated to build and iteratively refine the programme theory and finalise it for testing.
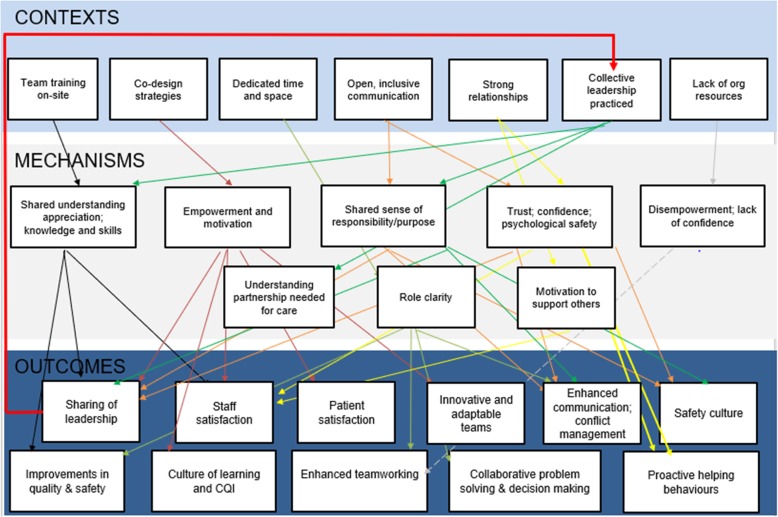
Twelve CMOCs were extrapolated from these data to form the initial programme theory and seven were prioritised by the expert panel for focused testing. Contextual conditions that emerged included team training on-site, use of collaborative/co-design strategies, dedicated time for team reflection on performance, organisational and senior management support, inclusive communication and decision-making processes and strong supportive interpersonal relationships within teams. Mechanisms reported include motivation, empowerment, role clarity, feeling supported and valued and psychological safety which led to outcomes including improvements in quality and safety, staff and patient satisfaction, enhanced team working, and greater willingness to share and adopt leadership roles and responsibilities.
This study has identified preliminary support for the contexts, mechanisms and outcomes underpinning the practice of collective leadership. However, it must be noted that while they may appear linear in presentation, in reality they are independent and interlinked and generative of additional configurations. This paper contributes to the nascent literature through addressing an identified gap in knowledge by penetrating below the surface level inputs and outputs of an intervention to understand why it works or doesn't work, and for whom it may work.
越来越多的证据表明,集体和共享的领导方法具有价值。然而,相对较少的研究探索了医疗保健中的集体领导,因此,对于促进或抑制医疗保健团队中集体领导实践的机制缺乏了解。本研究描述了初始方案理论(IPT)的发展,以深入了解集体领导实践的基础机制。
该 IPT 是通过对医疗保健环境中集体领导干预措施的文献进行综合现实主义研究(n=21 项研究)而得出的。接下来,我们向现实主义研究同行支持小组展示了初步结果,以征求反馈意见。然后对被确定为集体工作的团队成员(n=23)进行访谈,最后与专家小组(n=5)进行协商。从这些数据中推断出了上下文-机制-结果配置(CMOC),以构建和迭代完善方案理论,并为测试做好准备。
从这些数据中推断出了 12 个 CMOC,形成了初始方案理论,其中 7 个被专家小组优先进行了重点测试。出现的背景条件包括现场团队培训、使用协作/共同设计策略、为团队对绩效进行反思留出专门时间、组织和高级管理层的支持、包容的沟通和决策过程以及团队内部牢固的支持性关系。报告的机制包括动机、赋权、角色明确、感到支持和重视以及心理安全,这些机制导致了质量和安全性提高、员工和患者满意度提高、团队合作增强以及更愿意分享和承担领导角色和责任等结果。
本研究初步支持了集体领导实践的背景、机制和结果。然而,必须指出的是,虽然它们在呈现上可能是线性的,但实际上它们是独立的、相互关联的,并且可以产生其他配置。本文通过深入了解干预措施的表面投入和产出背后的原因,解决了知识中的一个已知差距,为新兴文献做出了贡献,以了解为什么它有效或无效,以及对谁有效。