Department of Scientific Computing and Numerical Analysis, Simula Research Laboratory, Lysaker, Norway.
Department of Radiation Sciences, Umeå University, Umeå, Sweden.
Fluids Barriers CNS. 2020 Apr 16;17(1):29. doi: 10.1186/s12987-020-00189-1.
Infusion testing is a common procedure to determine whether shunting will be beneficial in patients with normal pressure hydrocephalus. The method has a well-developed theoretical foundation and corresponding mathematical models that describe the CSF circulation from the choroid plexus to the arachnoid granulations. Here, we investigate to what extent the proposed glymphatic or paravascular pathway (or similar pathways) modifies the results of the traditional mathematical models.
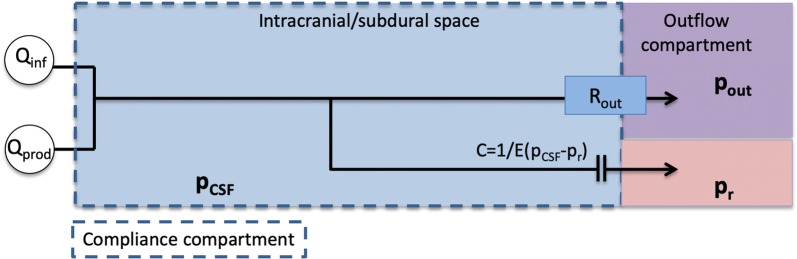
We used a compartment model to estimate pressure in the subarachnoid space and the paravascular spaces. For the arachnoid granulations, the cribriform plate and the glymphatic circulation, resistances were calculated and used to estimate pressure and flow before and during an infusion test. Finally, different variations to the model were tested to evaluate the sensitivity of selected parameters.
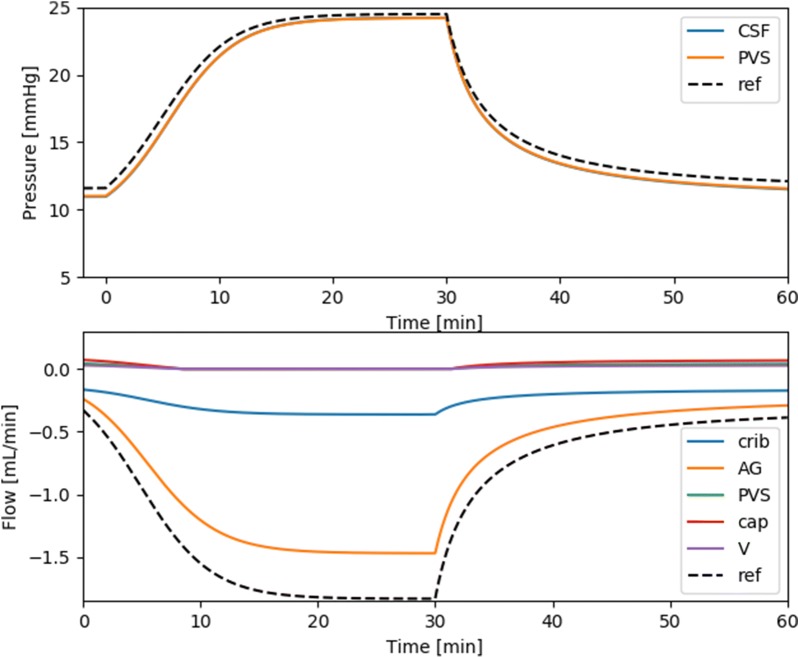
At baseline intracranial pressure (ICP), we found a very small paravascular flow directed into the subarachnoid space, while 60% of the fluid left through the arachnoid granulations and 40% left through the cribriform plate. However, during the infusion, 80% of the fluid left through the arachnoid granulations, 20% through the cribriform plate and flow in the PVS was stagnant. Resistance through the glymphatic system was computed to be 2.73 mmHg/(mL/min), considerably lower than other fluid pathways, giving non-realistic ICP during infusion if combined with a lymphatic drainage route.
The relative distribution of CSF flow to different clearance pathways depends on ICP, with the arachnoid granulations as the main contributor to outflow. As such, ICP increase is an important factor that should be addressed when determining the pathways of injected substances in the subarachnoid space. Our results suggest that the glymphatic resistance is too high to allow for pressure driven flow by arterial pulsations and at the same time too small to allow for a direct drainage route from PVS to cervical lymphatics.
输注测试是一种常见的程序,用于确定分流是否对正常压力脑积水患者有益。该方法具有成熟的理论基础和相应的数学模型,用于描述从脉络丛到蛛网膜颗粒的 CSF 循环。在这里,我们研究了提出的糖质或脉络丛途径(或类似途径)在多大程度上改变了传统数学模型的结果。
我们使用一个隔室模型来估计蛛网膜下腔和脉络丛空间的压力。对于蛛网膜颗粒、筛板和糖质循环,计算了阻力并用于在输注测试之前和期间估计压力和流量。最后,测试了模型的不同变体,以评估选定参数的敏感性。
在基础颅内压 (ICP) 下,我们发现有非常小的脉络丛流进入蛛网膜下腔,而 60%的液体通过蛛网膜颗粒离开,40%通过筛板离开。然而,在输注过程中,80%的液体通过蛛网膜颗粒离开,20%通过筛板离开,而 PVS 中的血流停滞。计算得出糖质系统的阻力为 2.73mmHg/(mL/min),远低于其他液体途径,如果与淋巴引流途径结合,会导致输注过程中 ICP 不真实。
CSF 流到不同清除途径的相对分布取决于 ICP,蛛网膜颗粒是流出的主要贡献者。因此,当确定蛛网膜下腔注射物质的途径时,ICP 增加是一个重要因素。我们的结果表明,糖质阻力太高,无法允许动脉搏动驱动的压力驱动流动,同时太小,无法允许从 PVS 到颈淋巴的直接引流途径。