Department of Epidemiology and Global health, Umeå University, Umeå, Västerbotten, SE.
Children's National Health System, Washington, DC, US.
Glob Heart. 2020 Feb 20;15(1):18. doi: 10.5334/gh.529.
In recent years, new technologies - noticeably ultra-portable echocardiographic machines - have emerged, allowing for Rheumatic Heart Disease (RHD) early diagnosis. We aimed to perform a cost-utility analysis to assess the cost-effectiveness of RHD screening with handheld devices in the Brazilian context.
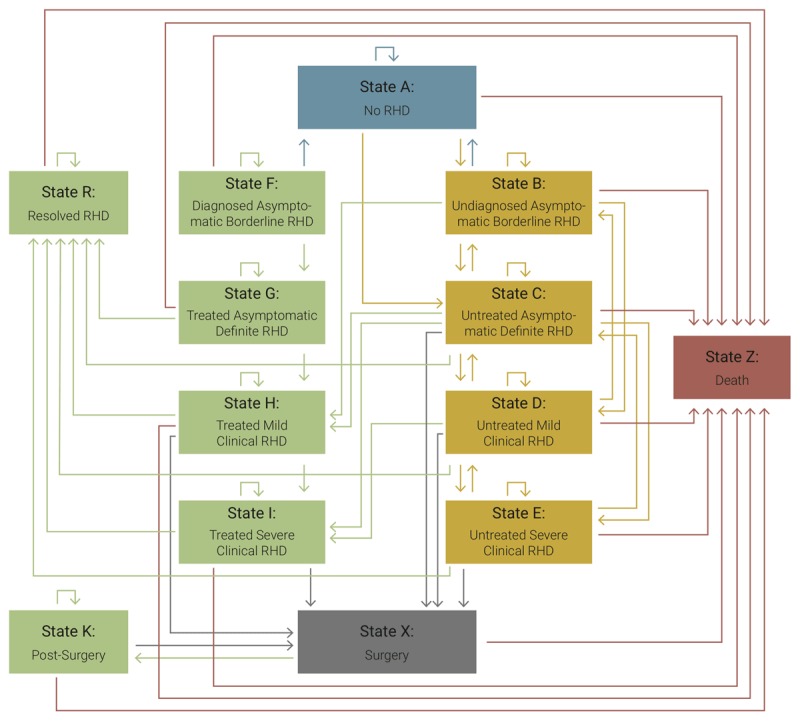
A Markov model was created to assess the cost-effectiveness of one-time screening for RHD in a hypothetical cohort of 11-year-old socioeconomically disadvantaged children, comparing the intervention to standard care using a public perspective and a 30-year time horizon. The model consisted of 13 states: No RHD, Undiagnosed Asymptomatic Borderline RHD, Diagnosed Asymptomatic Borderline RHD, Untreated Asymptomatic Definite RHD, Treated Asymptomatic Definite RHD, Untreated Mild Clinical RHD, Treated Mild Clinical RHD, Untreated Severe Clinical RHD, Treated Severe Clinical RHD, Surgery, Post-Surgery and Death. The initial distribution of the population over the different states was derived from primary echo screening data. Costs of the different states were derived from the Brazilian public health system database. Transition probabilities and utilities were derived from published studies. A discount rate of 3%/year was used. A cost-effectiveness threshold of $25,949.85 per Disability Adjusted Life Year (DALY) averted is used in concordance with the 3x GDP per capita threshold in 2015.
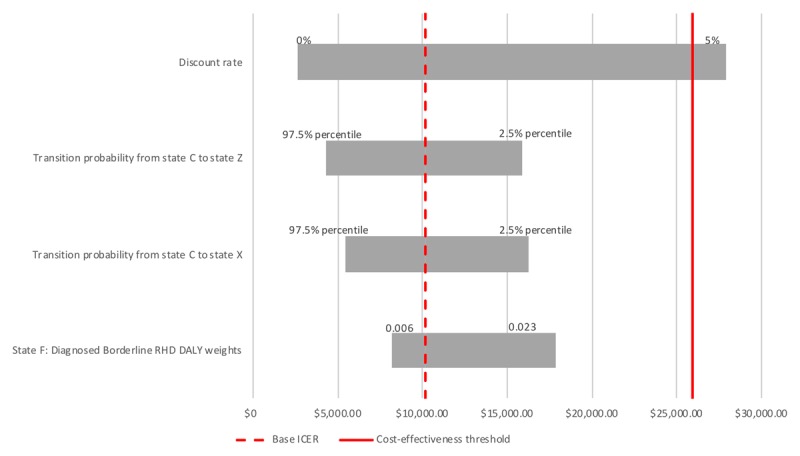
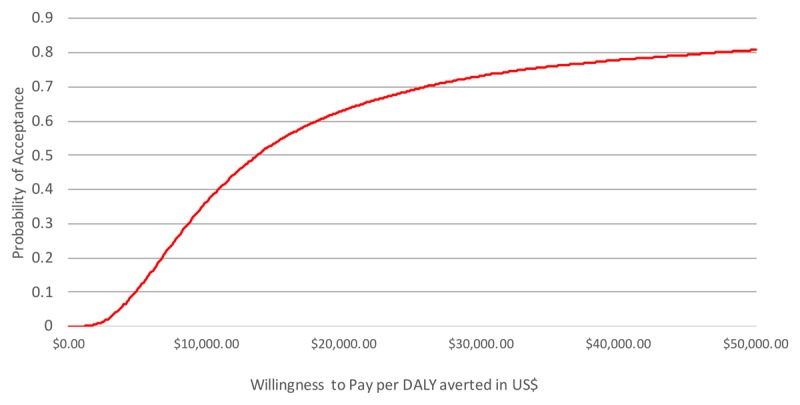
RHD echo screening is cost-effective with an Incremental Cost-Effectiveness Ratio of $10,148.38 per DALY averted. Probabilistic modelling shows that the intervention could be considered cost-effective in 70% of the iterations.
Screening for RHD with hand held echocardiographic machines in 11-year-old children in the target population is cost-effective in the Brazilian context.
A cost-effectiveness analysis showed that Rheumatic Heart Disease (RHD) echocardiographic screening utilizing handheld devices, performed by non-physicians with remote interpretation by telemedicine is cost-effective in a 30-year time horizon in Brazil.The model included primary data from the first large-scale RHD screening program in Brazilian underserved populations and costs from the Unified Health System (SUS), and suggests that the Incremental Cost-Effectiveness Ratio of the intervention is considerably below the acceptable threshold for Brazil, even after a detailed sensitivity analysis.Considering the high prevalence of subclinical RHD in Brazil, and the significant economic burden posed by advanced disease, these data are important for the formulation of public policies and surveillance approaches.Cost-saving strategies first implemented in Brazil by the PROVAR study, such as task-shifting to non-physicians, computer-based training, routine use of affordable devices and telemedicine for remote diagnosis may help planning RHD control programs in endemic areas worldwide.
近年来,新技术——尤其是超便携超声心动图机——的出现,使得风湿性心脏病(Rheumatic Heart Disease,RHD)的早期诊断成为可能。我们旨在进行成本效用分析,以评估在巴西背景下使用手持式设备进行 RHD 筛查的成本效益。
创建了一个马尔可夫模型,以评估在假设的 11 岁社会经济弱势群体儿童队列中进行一次性 RHD 筛查的成本效益,使用公共视角和 30 年时间范围比较干预措施与标准护理。该模型由 13 个状态组成:无 RHD、无症状边界性 RHD 未确诊、无症状边界性 RHD 确诊、无症状确定性 RHD 未经治疗、无症状确定性 RHD 经治疗、无症状轻度临床 RHD 未经治疗、无症状轻度临床 RHD 经治疗、无症状严重临床 RHD 未经治疗、无症状严重临床 RHD 经治疗、手术、手术后和死亡。人群在不同状态下的初始分布源自初级超声筛查数据。不同状态的成本来自巴西公共卫生系统数据库。转移概率和效用来自已发表的研究。使用 3%/年的贴现率。与 2015 年 3 倍人均 GDP 阈值一致,将避免每残疾调整生命年(Disability Adjusted Life Year,DALY)的成本效益阈值设定为 25,949.85 美元。
RHD 超声筛查具有成本效益,增量成本效益比为每避免 1 个 DALY 为 10,148.38 美元。概率模型表明,该干预措施在 70%的迭代中可能具有成本效益。
在巴西目标人群中,对 11 岁儿童进行手持式超声心动图筛查以筛查 RHD 具有成本效益。
成本效益分析表明,在巴西,利用手持式设备对非专业人员进行远程解释的远程医疗进行风湿性心脏病(RHD)超声筛查,在 30 年时间范围内具有成本效益。该模型纳入了巴西服务不足人群首次大规模 RHD 筛查计划的原始数据和统一卫生系统(SUS)的成本,并表明该干预措施的增量成本效益比远低于巴西的可接受阈值,即使在详细的敏感性分析之后也是如此。考虑到巴西亚临床 RHD 的高患病率以及晚期疾病带来的巨大经济负担,这些数据对于制定公共政策和监测方法非常重要。巴西 PROVAR 研究首先实施的成本节约策略,例如向非医生转移任务、基于计算机的培训、常规使用负担得起的设备和远程诊断的远程医疗,可能有助于规划全球流行地区的 RHD 控制计划。