Shah Sanchi, Shah Shimoni, Rangan Sheela, Rai Sonukumar, Lobo Eunice, Kamble Swaran, Dholakia Yatin, Mistry Nerges
The Foundation for Medical Research, Mumbai, India.
Gates Open Res. 2020 Apr 9;4:32. doi: 10.12688/gatesopenres.13113.1. eCollection 2020.
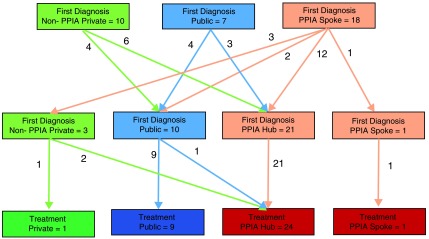
Public-private interface agency (PPIA) intervention models in Patna (E. India) and Mumbai (W. India) for pulmonary drug-sensitive (DS) tuberculosis (TB) patients were evaluated over 2 years after maturity to examine effect on reduction of patient pathways and retention. The models engaged private providers, diagnostic facilities and pharmacies into an effective network providing free diagnostic tests and treatment. A population-based retrospective study was undertaken to assess effectiveness of the PPIA model in care pathways of 64 (Patna) and 86 (Mumbai) patients through in-depth interviews conducted within 6 months of initiation treatments to identify types and facilities accessed, duration to diagnosis and treatment. Median durations based on facilities accessed were statistically analysed. Comparisons were made with baseline values and endline pathways of patients accessing PPIA engaged/non-engaged facilities in private and public sectors. Compared to non-engaged facilities, persons accessing engaged facilities at first point-of-care had shorter pathways (Mumbai: 32 vs 43 days), (Patna: 15 vs 40 days). Duration for first care-seeking was considerably shorter for patients accessing PPIA in Patna and for both engaged and non-engaged private facilities in Mumbai (4 days). Whilst PPIA engaged facilities diagnosed more cases than others, the RNTCP in Mumbai provided diagnosis early. There was good retention of patients by PPIA-engaged (1 ) facilities (90% post-diagnosis in Patna) but this was affected by the hub-spoke referral system in Mumbai (13%). Second diagnosis is a common feature in Mumbai. The spoke-hub model in Mumbai contributed considerably to treatment delay; PPIA-engaged providers were better at retaining patients post treatment initiation 11/25 (44%). PPIA-engaged facilities, accessed at onset, result in marked reduction in pathway durations. Such initiatives should engage a critical mass of competent providers, proximal investigation facilities with enhanced disease awareness and literacy efforts amongst communities. Patient movement should be minimized for early treatment and retention.
对印度东部巴特那和西部孟买针对肺结核药物敏感(DS)患者的公私合作接口机构(PPIA)干预模式在成熟后的两年内进行了评估,以考察其对减少患者就医流程和提高留存率的影响。这些模式让私立医疗服务提供者、诊断机构和药房形成一个有效的网络,提供免费诊断测试和治疗。开展了一项基于人群的回顾性研究,通过在开始治疗后的6个月内进行深入访谈,以评估PPIA模式在64名(巴特那)和86名(孟买)患者就医流程中的有效性,从而确定他们使用的医疗服务类型和机构、诊断和治疗所需时间。对基于所使用机构的中位时长进行了统计分析。将其与在公私部门中使用PPIA合作/未合作机构的患者的基线值和最终就医流程进行了比较。与未合作机构相比,在首次就医时使用合作机构的患者就医流程更短(孟买:32天对43天),(巴特那:15天对40天)。在巴特那使用PPIA的患者以及在孟买使用合作和未合作私立机构的患者首次寻求医疗服务的时长都显著更短(4天)。虽然PPIA合作机构诊断出的病例比其他机构多,但孟买的印度修订国家结核病控制规划(RNTCP)能更早做出诊断。PPIA合作机构对患者的留存情况良好(巴特那诊断后为90%),但这受到孟买中心-辐射转诊系统的影响(13%)。二次诊断在孟买很常见。孟买的辐射-中心模式对治疗延迟有很大影响;PPIA合作的医疗服务提供者在治疗开始后对患者的留存情况更好,为11/25(44%)。一开始就使用PPIA合作机构可显著缩短就医流程时长。此类举措应吸引大量有能力的医疗服务提供者、具备疾病意识提升和社区宣传能力的近端调查机构参与。应尽量减少患者流动以实现早期治疗和提高留存率。