Department of Health Metrics Sciences, University of Washington, Institute for Health Metrics and Evaluation, Seattle, Washington, USA.
Medtronic Foundation, Minneapolis, Minnesota, USA.
BMJ Glob Health. 2020 Jun;5(6). doi: 10.1136/bmjgh-2019-001959.
As non-communicable disease (NCD) burden rises worldwide, community-based programmes are a promising strategy to bridge gaps in NCD care. The HealthRise programme sought to improve hypertension and diabetes management for underserved communities in nine sites across Brazil, India, South Africa and the USA between 2016 and 2018. This study presents findings from the programme's endline evaluation.
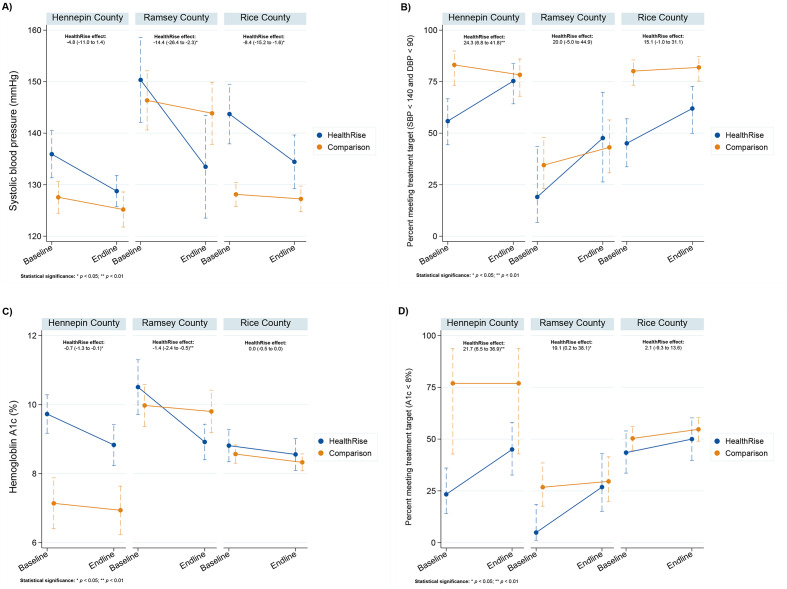
The evaluation utilises a mixed-methods quasi-experimental design. Process indicators assess programme implementation; quantitative data examine patients' biometric measures and qualitative data characterise programme successes and challenges. Programme impact was assessed using the percentage of patients meeting blood pressure and A1c treatment targets and tracking changes in these measures over time.
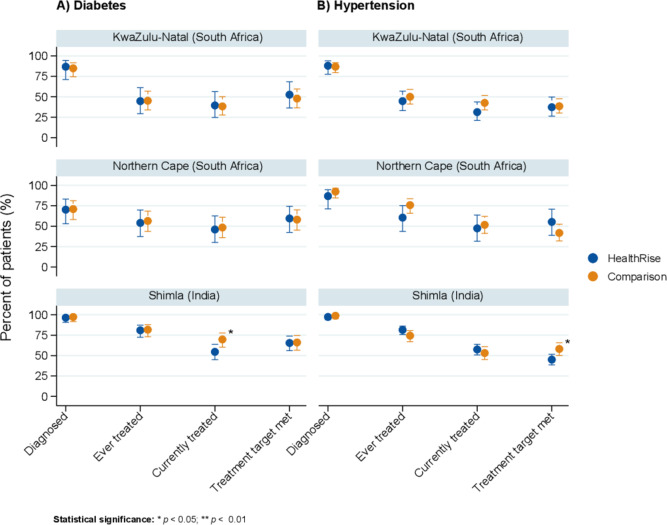
Almost 60 000 screenings, most of them in India, resulted in 1464 new hypertension and 295 new diabetes cases across sites. In Brazil, patients exhibited statistically significant reductions in blood pressure and A1c. In Shimla, India, and in South Africa, country with the shortest implementation period, there were no differences between patients served by facilities in HealthRise areas relative to comparison areas. Among participating patients with diabetes in Hennepin and Ramsey counties and hypertension patients in Hennepin County, the percentage of HealthRise patients meeting treatment targets at endline was significantly higher relative to comparison group patients. Qualitative analysis identified linking different providers, services, communities and information systems as positive HealthRise attributes. Gaps in health system capacities and sociodemographic factors, including poverty, low levels of health education and limited access to nutritious food, are remaining challenges.
Findings from Brazil and the USA indicate that the HealthRise model has the potential to improve patient outcomes. Short implementation periods and strong emphasis on screening may have contributed to the lack of detectable differences in other sites. Community-based care cannot deliver its full potential if sociodemographic and health system barriers are not addressed in tandem.
随着全球非传染性疾病(NCD)负担的增加,以社区为基础的方案是弥合 NCD 护理差距的一种有前途的策略。HealthRise 计划旨在改善巴西、印度、南非和美国 9 个地点的服务不足社区的高血压和糖尿病管理,时间为 2016 年至 2018 年。本研究介绍了该计划的终线评估结果。
该评估采用混合方法准实验设计。过程指标评估方案实施情况;定量数据检查患者的生物计量指标,定性数据描述方案的成功和挑战。使用符合血压和 A1c 治疗目标的患者比例以及随时间推移这些指标的变化来评估方案的影响。
近 60000 次筛查,其中大部分在印度进行,导致 9 个地点的新高血压和新糖尿病病例分别为 1464 例和 295 例。在巴西,患者的血压和 A1c 显著降低。在印度的希姆拉和南非(实施时间最短的国家),HealthRise 服务区域内的患者与对照区域内的患者之间没有差异。在亨内平县和拉姆齐县的参与糖尿病患者和亨内平县的高血压患者中,符合治疗目标的 HealthRise 患者比例显著高于对照组患者。定性分析确定了将不同的提供者、服务、社区和信息系统联系起来是 HealthRise 的积极属性。卫生系统能力和社会人口因素方面的差距,包括贫困、健康教育水平低以及获得营养食品的机会有限,仍然是挑战。
来自巴西和美国的研究结果表明,HealthRise 模式有可能改善患者的治疗效果。较短的实施期和对筛查的高度重视可能导致其他地点没有检测到差异。如果不同步解决社会人口和卫生系统障碍,以社区为基础的护理就无法充分发挥其潜力。