Medical Student Research Office, Icahn School of Medicine at Mount Sinai, New York, New York, USA.
Brookdale Department of Geriatrics and Palliative Medicine, Icahn School of Medicine at Mount Sinai, New York, New York, USA.
J Am Geriatr Soc. 2020 Oct;68(10):2288-2296. doi: 10.1111/jgs.16648. Epub 2020 Jun 30.
BACKGROUND/OBJECTIVES: Hospice care confers well-documented benefits to patients and their families, but it is underutilized. One potential reason is inadequate family support to make end-of-life decisions and care for older adults on hospice at home. We assessed the association between amount of family support and hospice use among a population of decedents and among specific illness types.
Prospective cohort study using the National Health and Aging Trends Study waves 2011 to 2017, linked to Medicare claims data.
Contiguous United States.
A total of 1,868 NHATS decedents.
Outcome variable was 1 day or longer of hospice. Family caregiving intensity was measured by self-reported hours of care per week and number of caregivers. Covariates included probable dementia status and other demographic, clinical, and functional characteristics.
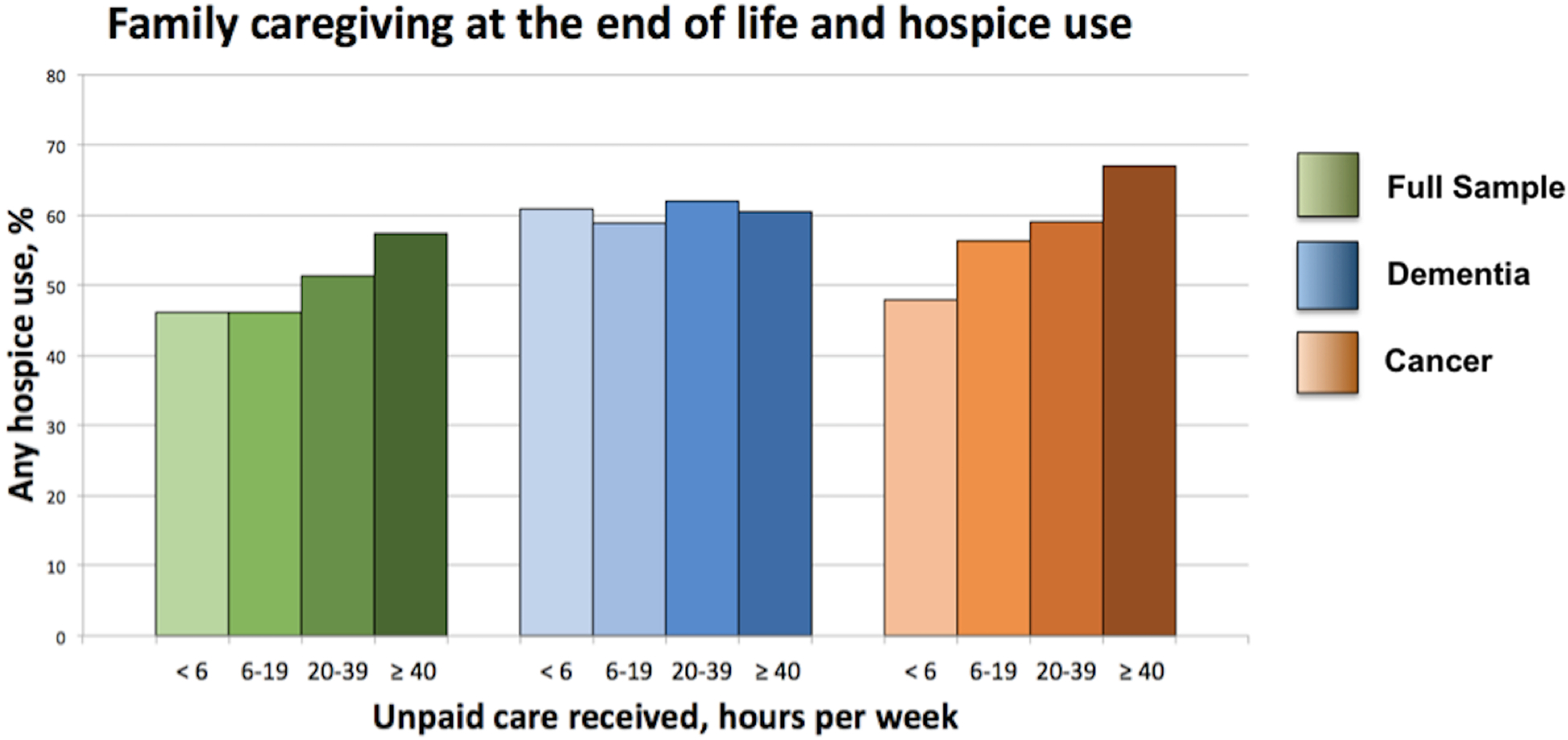
At the end of life, hours of family caregiving and numbers of helpers vary widely with individuals with dementia receiving the most hours of unpaid care (mean = 64.5 hours per week) and having 2.4 unpaid caregivers on average. In an adjusted analysis, older adults with cancer receiving 40 hours and more of unpaid care/week as compared with fewer than 6 hours per week were twice as likely to receive hospice care at the end of life (odds ratio = 2.0; 95% confidence interval = 1.0-4.1). This association was not seen among those with dementia or among decedents in general. No significant association was found between number of caregivers and hospice use at the end of life.
Older adults at the end of life receive a high number of hours of help at the end of life, many from more than one caregiver, which may shape hospice access. Better understanding of disparities in hospice use can facilitate timely access to care for older adults with a serious illness. J Am Geriatr Soc 68:2288-2296, 2020.
背景/目的:临终关怀为患者及其家属带来了有据可查的益处,但它的利用率却很低。一个潜在的原因是,家庭成员在做出临终决策和在家中照顾老年人方面的支持不足。我们评估了在一个死者人群中和特定疾病类型中,家庭支持的数量与使用临终关怀之间的关联。
使用 2011 年至 2017 年的国家健康老龄化趋势研究(National Health and Aging Trends Study)波次进行前瞻性队列研究,并与医疗保险索赔数据相关联。
美国大陆。
共有 1868 名 NHATS 死者。
因变量为接受临终关怀 1 天或以上。家庭护理强度通过自我报告的每周护理小时数和护理人员数量来衡量。协变量包括可能的痴呆状况以及其他人口统计学、临床和功能特征。
在生命的尽头,家庭护理的时间和护理人员的数量因人而异,患有痴呆症的个体接受的无薪护理时间最长(平均每周 64.5 小时),平均有 2.4 名无薪护理人员。在调整后的分析中,与每周接受少于 6 小时的无薪护理相比,癌症患者每周接受 40 小时或更多的无薪护理/周的患者在生命结束时接受临终关怀的可能性是前者的两倍(优势比=2.0;95%置信区间=1.0-4.1)。在痴呆症患者或一般死者中,没有发现护理人员数量与临终关怀使用之间存在显著关联。
生命末期的老年人在生命末期会得到大量的帮助,其中许多来自不止一个护理人员,这可能会影响临终关怀的获得。更好地了解临终关怀使用方面的差异,可以为患有严重疾病的老年人提供及时的护理。美国老年学会杂志 68:2288-2296,2020 年。