Ko Young Hwii, Huynh Linda My, See Kaelyn, Lall Chandana, Skarecky Douglas, Ahlering Thomas E
Department of Urology, Yeoungnam University, Daegu, Korea.
Department of Urology, University of California, Irvine Medical Center, Orange, CA, USA.
Prostate Int. 2020 Jun;8(2):55-61. doi: 10.1016/j.prnil.2019.12.005. Epub 2020 Mar 7.
Pelvic multiparametric magnetic resonance imaging (mpMRI)-determined membranous urethral length (MUL) and its surgical maximization have been reported to impact early- and long-term pad-free urinary continence after robot-assisted radical prostatectomy (RARP).
The objective of this study was to present evidence (data and video) of important effects on post-RARP continence recovery from both innate mpMRI-assessed and surgical preservation of MUL.
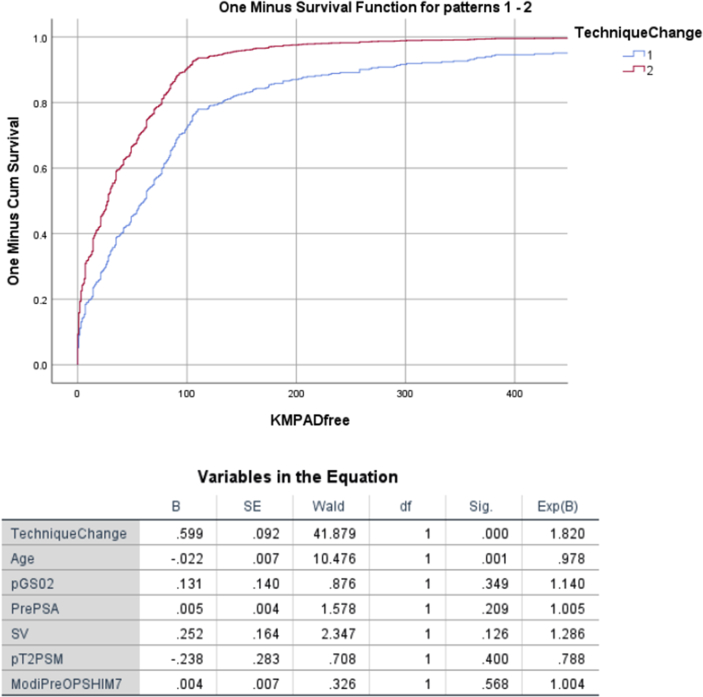
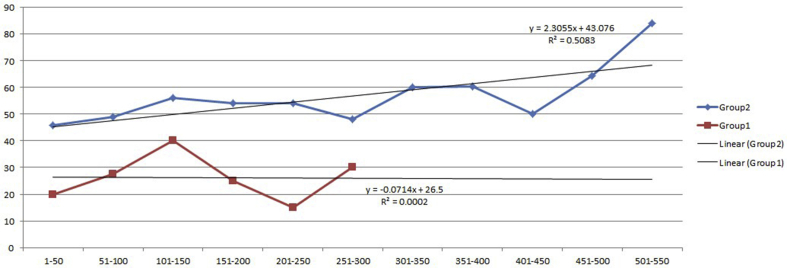
Of 605 men undergoing RARP, 580 with complete follow-up were included: Group 1, prior (N = 355), and Group 2, subsequent (N = 225) to technique change of MUL maximization. Effect of innate, mpMRI-assessed MUL on postoperative continence was assessed.
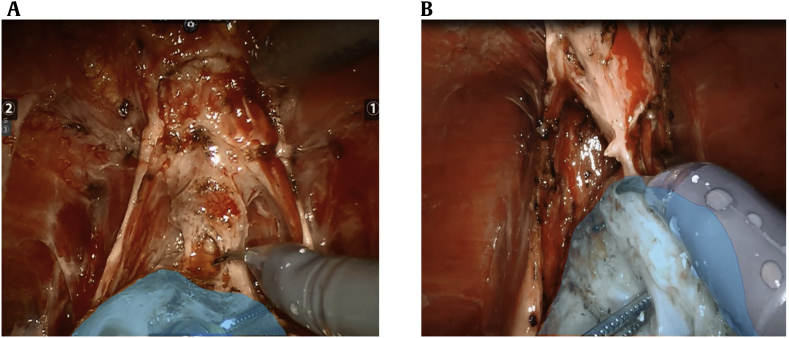
Before technique change, the dorsal venous complex was stapled before transection of the membranous urethra. After the change, the final step of extirpation was transection of the dorsal venous complex and periurethral attachments, thus facilitating surgical maximization of MUL.
Primary and secondary outcomes for technique change and mpMRI-assessed MUL were both patient-reported 30-day and 1-year pad-free continence after RARP, respectively.
Preoperative prostate-specific antigen, age, and disease aggressiveness were significantly higher in Group 2. After technique change and surgical maximization of MUL, 30-day and 1-year pad-free continence were both significantly improved ( < 0.05). In multivariate analysis, maximization of MUL significantly increased the likelihood of both early- and long-term continence recovery. For men undergoing MUL preservation, mpMRI-assessed MUL>1.4 cm also independently predicted higher 30-day (odds ratio: 4.85, 95% confidence interval: 1.24-18.9) and 1-year continence recovery (odds ratio: 11.26, 95% confidence interval: 1.07-118).
Prostatic rotation and circumferential release of apical attachments and maximization of MUL improves continence after RARP. Separately, innate MUL>1.4 cm independently increased 30-day and 1-year continence recovery.
Surgeon efforts to maximize MUL during radical prostatectomy are highly encouraged, as maximally preserved MUL likely improves post-RARP continence recovery. In addition, individual patients' mpMRI-assessed MUL (approximately >1.4 cm) independently limits continence recovery.
据报道,盆腔多参数磁共振成像(mpMRI)测定的膜性尿道长度(MUL)及其手术最大化对机器人辅助根治性前列腺切除术(RARP)后的早期和长期无垫尿控有影响。
本研究的目的是提供证据(数据和视频),证明先天性mpMRI评估和手术保留MUL对RARP后控尿恢复的重要影响。
设计、设置和参与者:在605例行RARP的男性中,纳入580例有完整随访资料的患者:第1组,在MUL最大化技术改变之前(N = 355),第2组,在MUL最大化技术改变之后(N = 225)。评估先天性mpMRI评估的MUL对术后控尿的影响。
在技术改变之前,在横断膜性尿道之前对背静脉复合体进行吻合钉合。改变之后,切除的最后一步是横断背静脉复合体和尿道周围附着组织,从而有利于MUL的手术最大化。
技术改变和mpMRI评估的MUL的主要和次要结局分别是患者报告的RARP术后30天和1年无垫尿控情况。
第2组患者术前前列腺特异性抗原、年龄和疾病侵袭性显著更高。在技术改变和MUL手术最大化之后,30天和1年无垫尿控情况均显著改善(P < 0.05)。在多变量分析中,MUL最大化显著增加了早期和长期控尿恢复的可能性。对于接受MUL保留的男性,mpMRI评估的MUL>1.4 cm也独立预测了更高的30天(比值比:4.85,95%置信区间:1.24 - 18.9)和1年控尿恢复率(比值比:11.26,95%置信区间:1.07 - 118)。
前列腺旋转、尖部附着组织的环形松解以及MUL最大化可改善RARP后的控尿情况。另外,先天性MUL>1.4 cm独立增加了30天和1年控尿恢复率。
强烈鼓励外科医生在根治性前列腺切除术中努力使MUL最大化,因为最大程度保留MUL可能会改善RARP后的控尿恢复情况。此外,个体患者mpMRI评估的MUL(约>1.4 cm)独立限制控尿恢复情况。