Department of Pulmonary and Critical Care Medicine, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Republic of Korea.
Big Data & AI Lab, Hana Institute of Technology, Hana TI, Seoul, Republic of Korea.
J Med Internet Res. 2020 Aug 4;22(8):e19512. doi: 10.2196/19512.
Detecting bacteremia among surgical in-patients is more obscure than other patients due to the inflammatory condition caused by the surgery. The previous criteria such as systemic inflammatory response syndrome or Sepsis-3 are not available for use in general wards, and thus, many clinicians usually rely on practical senses to diagnose postoperative infection.
This study aims to evaluate the performance of continuous monitoring with a deep learning model for early detection of bacteremia for surgical in-patients in the general ward and the intensive care unit (ICU).
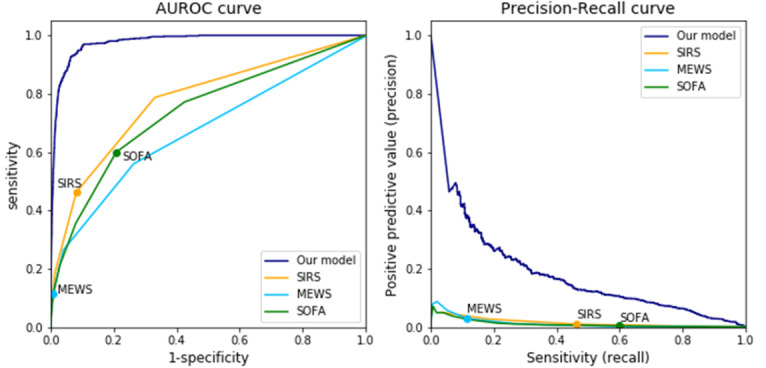
In this retrospective cohort study, we included 36,023 consecutive patients who underwent general surgery between October and December 2017 at a tertiary referral hospital in South Korea. The primary outcome was the area under the receiver operating characteristic curve (AUROC) and the area under the precision-recall curve (AUPRC) for detecting bacteremia by the deep learning model, and the secondary outcome was the feature explainability of the model by occlusion analysis.
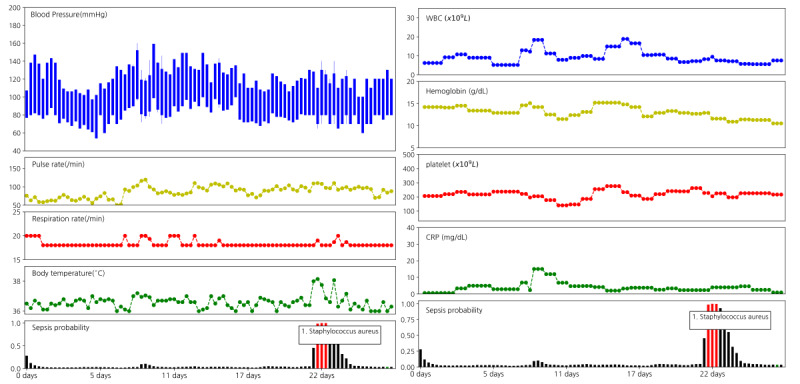
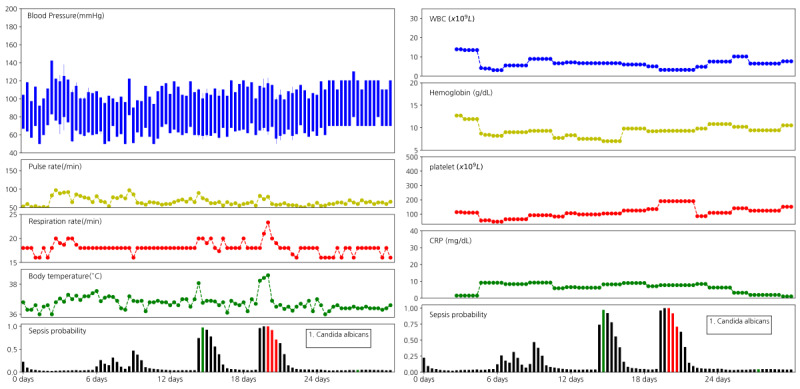
Out of the 36,023 patients in the data set, 720 cases of bacteremia were included. Our deep learning-based model showed an AUROC of 0.97 (95% CI 0.974-0.981) and an AUPRC of 0.17 (95% CI 0.147-0.203) for detecting bacteremia in surgical in-patients. For predicting bacteremia within the previous 24-hour period, the AUROC and AUPRC values were 0.93 and 0.15, respectively. Occlusion analysis showed that vital signs and laboratory measurements (eg, kidney function test and white blood cell group) were the most important variables for detecting bacteremia.
A deep learning model based on time series electronic health records data had a high detective ability for bacteremia for surgical in-patients in the general ward and the ICU. The model may be able to assist clinicians in evaluating infection among in-patients, ordering blood cultures, and prescribing antibiotics with real-time monitoring.
由于手术引起的炎症状态,外科住院患者的菌血症检测比其他患者更为复杂。以前的标准,如全身炎症反应综合征或 Sepsis-3,不适用于普通病房,因此,许多临床医生通常依靠实际感觉来诊断术后感染。
本研究旨在评估深度学习模型对普通病房和重症监护病房(ICU)外科住院患者菌血症的早期检测性能。
在这项回顾性队列研究中,我们纳入了 2017 年 10 月至 12 月期间在韩国一家三级转诊医院接受普通外科手术的 36023 例连续患者。主要结局是深度学习模型检测菌血症的受试者工作特征曲线下面积(AUROC)和精度-召回曲线下面积(AUPRC),次要结局是通过闭塞分析对模型的特征可解释性。
在数据集的 36023 例患者中,有 720 例发生菌血症。我们基于深度学习的模型对外科住院患者菌血症的检测 AUROC 为 0.97(95%CI 0.974-0.981),AUPRC 为 0.17(95%CI 0.147-0.203)。对于预测前 24 小时内的菌血症,AUROC 和 AUPRC 值分别为 0.93 和 0.15。闭塞分析表明,生命体征和实验室测量(如肾功能试验和白细胞群)是检测菌血症的最重要变量。
基于时间序列电子健康记录数据的深度学习模型对普通病房和 ICU 外科住院患者的菌血症具有较高的检测能力。该模型可以帮助临床医生实时监测评估住院患者的感染情况、进行血培养和开具抗生素。