Division of General Internal Medicine, Department of Medicine , Baylor College of Medicine, Houston, TX, USA.
Center for Innovations in Quality, Effectiveness, and Safety (IQuESt), Michael E DeBakey VA Medical Center, Houston, TX, USA.
J Gen Intern Med. 2021 Feb;36(2):455-463. doi: 10.1007/s11606-020-06017-4. Epub 2020 Jul 22.
Many individuals with diabetes live in low- or middle-income settings. Glycemic control is challenging, particularly in resource-limited areas that face numerous healthcare barriers.
To compare HbA1c outcomes for individuals randomized to TIME, a Telehealth-supported, Integrated care with CHWs (Community Health Workers), and MEdication-access program (intervention) versus usual care (wait-list control).
Randomized clinical trial.
Low-income Latino(a) adults with type 2 diabetes.
TIME consisted of (1) CHW-participant telehealth communication via mobile health (mHealth) for 12 months, (2) CHW-led monthly group visits for 6 months, and (3) weekly CHW-physician diabetes training and support via telehealth (video conferencing).
Investigators compared TIME versus control participant baseline to month 6 changes of HbA1c (primary outcome), blood pressure, body mass index (BMI), weight, and adherence to seven American Diabetes Association (ADA) standards of care. CHW assistance in identifying barriers to healthcare in the intervention group were measured at the end of mHealth communication (12 months).
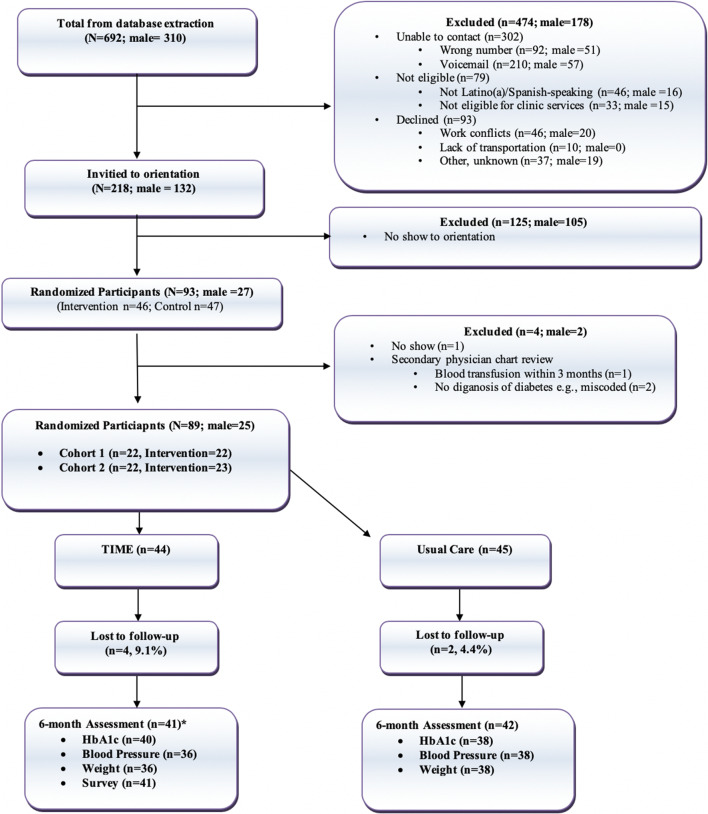
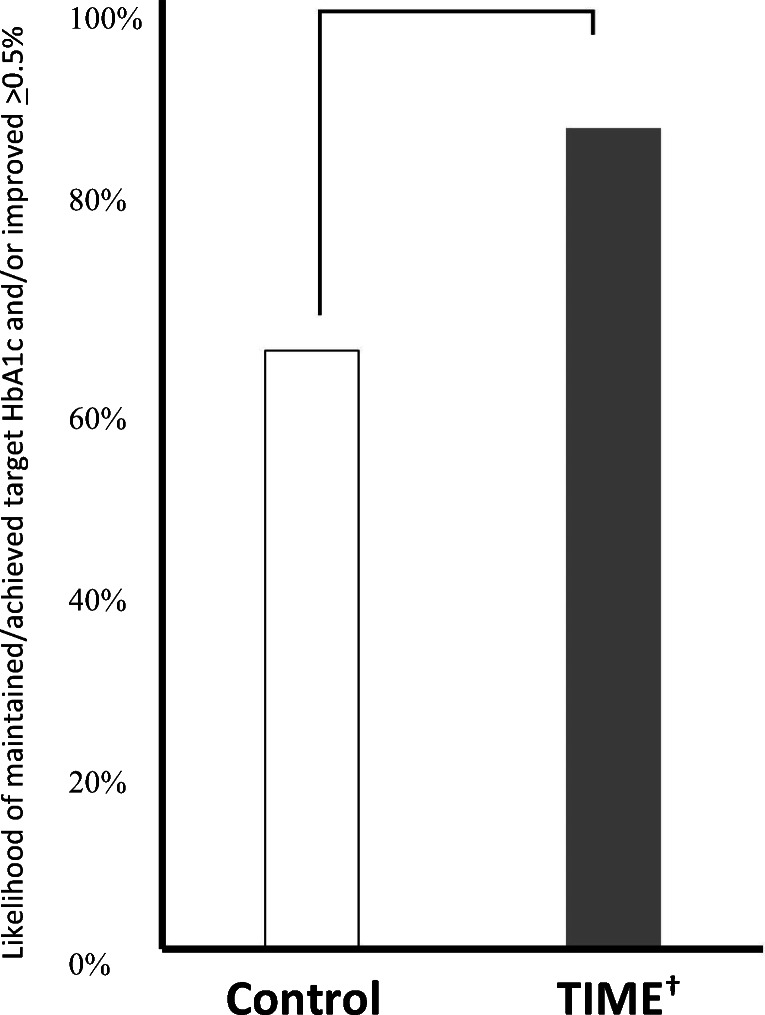
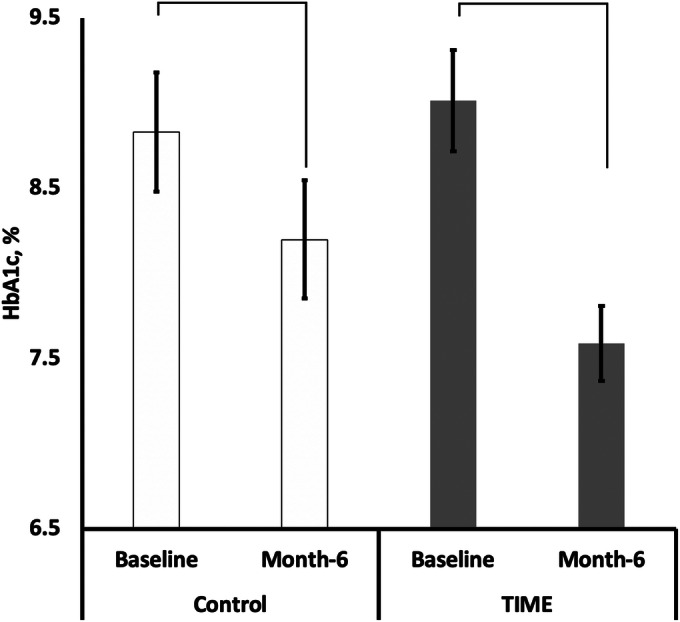
A total of 89 individuals participated. TIME individuals compared to control participants had significant HbA1c decreases (9.02 to 7.59% (- 1.43%) vs. 8.71 to 8.26% (- 0.45%), respectively, p = 0.002), blood pressure changes (systolic: - 6.89 mmHg vs. 0.03 mmHg, p = 0.023; diastolic: - 3.36 mmHg vs. 0.2 mmHg, respectively, p = 0.046), and ADA guideline adherence (p < 0.001) from baseline to month 6. At month 6, more TIME than control participants achieved > 0.50% HbA1c reductions (88.57% vs. 43.75%, p < 0.001). BMI and weight changes were not significant between groups. Many (54.6%) TIME participants experienced > 1 barrier to care, of whom 91.7% had medication issues. CHWs identified the majority (87.5%) of barriers.
TIME participants resulted in improved outcomes including HbA1c. CHWs are uniquely positioned to identify barriers to care particularly related to medications that may have gone unrecognized otherwise. Larger trials are needed to determine the scalability and sustainability of the intervention.
NCT03394456, accessed at https://clinicaltrials.gov/ct2/show/NCT03394456.
许多糖尿病患者生活在中低收入环境中。血糖控制具有挑战性,特别是在资源有限的地区,这些地区面临着许多医疗保健障碍。
比较随机分配到 TIME 组(远程医疗支持的综合护理,包括社区卫生工作者和药物获取计划)和常规护理组的个体的糖化血红蛋白(HbA1c)结果。
随机临床试验。
患有 2 型糖尿病的低收入拉丁裔成年人。
TIME 包括(1)通过移动健康(mHealth)进行 12 个月的 CHW-参与者远程健康沟通,(2)进行 6 个月的 CHW 主导的每月小组访问,以及(3)每周通过远程医疗(视频会议)进行 CHW-医生糖尿病培训和支持。
研究人员比较了 TIME 组与对照组参与者在基线时到第 6 个月时的 HbA1c(主要结局)、血压、体重指数(BMI)、体重和对美国糖尿病协会(ADA)七项护理标准的依从性的变化。在 mHealth 沟通结束时(12 个月),干预组中 CHW 协助确定医疗保健障碍。
共有 89 人参与。与对照组相比,TIME 组的 HbA1c 显著降低(9.02%降至 7.59%(-1.43%),8.71%降至 8.26%(-0.45%),p=0.002),血压变化(收缩压:-6.89mmHg 与 0.03mmHg,p=0.023;舒张压:-3.36mmHg 与 0.2mmHg,p=0.046),以及 ADA 指南的依从性(p<0.001)从基线到第 6 个月。在第 6 个月,与对照组相比,更多的 TIME 组参与者实现了>0.50%的 HbA1c 降低(88.57%比 43.75%,p<0.001)。两组的 BMI 和体重变化均无显著差异。许多(54.6%)TIME 参与者经历了>1 个护理障碍,其中 91.7%存在药物问题。CHWs 确定了大多数(87.5%)障碍。
TIME 组的参与者改善了包括 HbA1c 在内的结果。社区卫生工作者具有独特的优势,可以识别护理障碍,特别是与药物相关的障碍,这些障碍否则可能未被发现。需要更大规模的试验来确定干预措施的可扩展性和可持续性。
NCT03394456,可在 https://clinicaltrials.gov/ct2/show/NCT03394456 上查阅。