Department of Medicine, Surgery and Dentistry, Neuroscience Section, Centre for Neurodegenerative Diseases (CEMAND), University of Salerno, Salerno, Italy.
Department of Medicine, Faculty of Medicine, Chulalongkorn Centre of Excellence for Parkinson's Disease & Related Disorders, Chulalongkorn University and King Chulalongkorn Memorial Hospital, Thai Red Cross Society, Bangkok, Thailand.
Mov Disord. 2021 Mar;36(3):672-680. doi: 10.1002/mds.28382. Epub 2020 Nov 9.
No clinical trials have been specifically designed to compare medical treatments after surgery in Parkinson's disease (PD).
Study's objective was to compare the efficacy and safety of levodopa versus dopamine agonist monotherapy after deep brain stimulation (DBS) in PD.
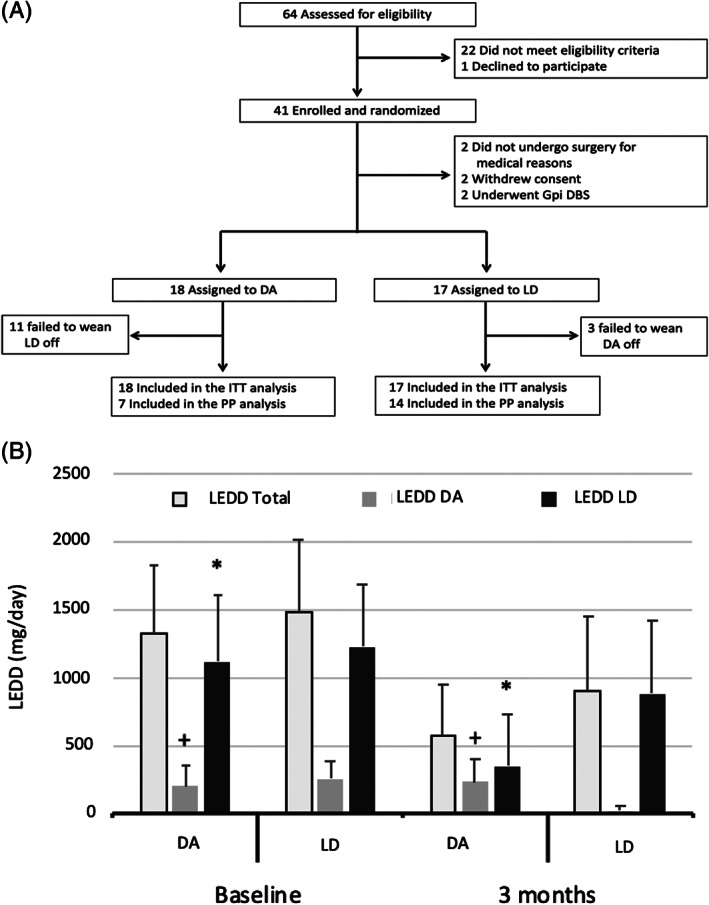
Thirty-five surgical candidates were randomly assigned to receive postoperative monotherapy with either levodopa or dopamine agonist in a randomized, single-blind study. All patients were reevaluated in short- (3 months), mid- (6 months), and long-term (2.5 years) follow-up after surgery. The primary outcome measure was the change in the Non-Motor Symptoms Scale (NMSS) 3 months after surgery. Secondary outcome measures were the percentage of patients maintaining monotherapy, change in motor symptoms, and specific non-motor symptoms (NMS). Analysis was performed primarily in the intention-to-treat population.
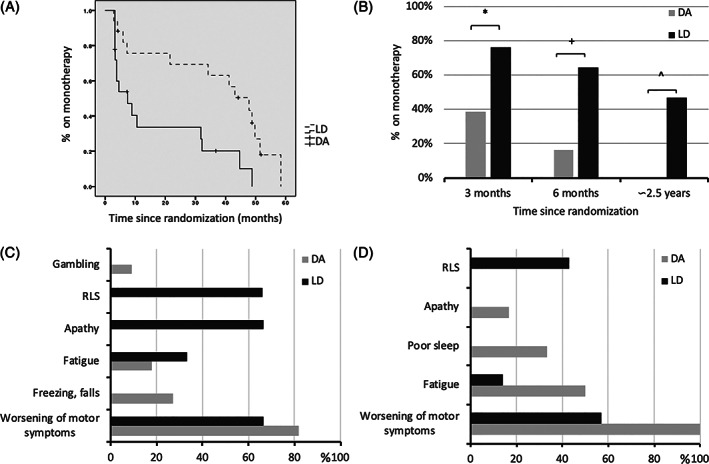
Randomization did not significantly affect the primary outcome (difference in NMSS between treatment groups was 4.88 [95% confidence interval: -11.78-21.53, P = 0.566]). In short- and mid-term follow-up, monotherapy was safe and feasible in more than half of patients (60% in short- and 51.5% in mid-term follow-up), but it was more often possible for patients on levodopa. The ability to maintain dopamine agonist monotherapy was related to optimal contact location. In the long term, levodopa monotherapy was feasible only in a minority of patients (34.2%), whereas dopamine agonist monotherapy was not tolerated due to worsening of motor conditions or occurrence of impulse control disorders.
This trial provides evidence for simplifying pharmacological treatment after functional neurosurgery for PD. The reduction in dopamine receptor agonists should be attempted while monitoring for occurrence of NMSs, such as apathy and sleep disturbances. © 2020 The Authors. Movement Disorders published by Wiley Periodicals LLC on behalf of International Parkinson and Movement Disorder Society.
目前尚无专门设计的临床试验来比较帕金森病(PD)术后的医学治疗方法。
本研究旨在比较深部脑刺激(DBS)后左旋多巴与多巴胺激动剂单药治疗在 PD 中的疗效和安全性。
35 名手术候选者被随机分配接受术后左旋多巴或多巴胺激动剂单药治疗,这是一项随机、单盲研究。所有患者在手术后的短期(3 个月)、中期(6 个月)和长期(2.5 年)随访中进行重新评估。主要结局指标是手术后 3 个月时非运动症状量表(NMSS)的变化。次要结局指标是维持单药治疗的患者比例、运动症状的变化以及特定的非运动症状(NMS)。分析主要在意向治疗人群中进行。
随机分组对主要结局无显著影响(治疗组之间 NMSS 的差异为 4.88[95%置信区间:-11.78-21.53,P=0.566])。在短期和中期随访中,超过一半的患者(短期随访中有 60%,中期随访中有 51.5%)接受单药治疗是安全且可行的,但接受左旋多巴治疗的患者比例更高。维持多巴胺激动剂单药治疗的能力与最佳接触位置有关。长期随访中,只有少数患者(34.2%)能够接受左旋多巴单药治疗,而由于运动状况恶化或出现冲动控制障碍,多巴胺激动剂单药治疗无法耐受。
本试验为简化 PD 功能性神经外科术后的药物治疗提供了证据。应尝试减少多巴胺受体激动剂的使用,同时监测是否出现淡漠和睡眠障碍等 NMS。