Eljilany Islam, Elzouki Abdel-Naser
Qatar University, College of Pharmacy, Doha, Qatar.
Hamad Medical Corporation, Hamad General Hospital, Department of Medicine, Doha, Qatar.
Vasc Health Risk Manag. 2020 Nov 13;16:455-462. doi: 10.2147/VHRM.S280962. eCollection 2020.
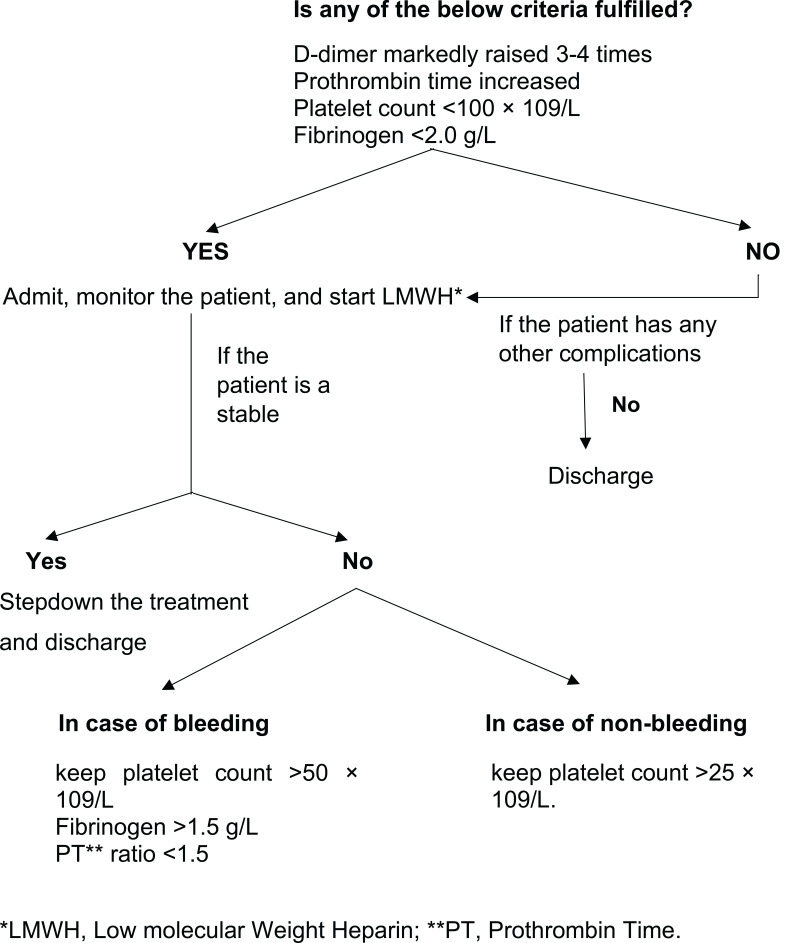
Coronavirus disease 2019 (COVID-19) emerged from the West District of Southern China Seafood Wholesale Market in late December 2019 and has been declared a global pandemic by the World Health Organization (WHO). Infection with severe acute respiratory syndrome coronavirus (SARS-CoV-2) presents with upper respiratory symptoms like cough, fever, and lethargy. At the same time, in later stages, critical COVID-19 patients develop acute respiratory distress syndrome (ARDS), venous thromboembolism (VTE), and multiple organ failure from cytokine storm and coagulation hyperactivity. Primary manifestations of thrombotic events include deep vein thrombosis (DVT), disseminated intravascular coagulation (DIC) and pulmonary embolism (PE). Initial coagulopathy in COVID-19 patients presents with elevated fibrin degradation products, especially D-dimers. In contrast, late presentations show evidence of prolonged prothrombin time (PT) and activated partial thromboplastin (aPTT), increased platelets, and fibrinogen levels. Diagnosis and monitoring of disease progression are done by regular screening of laboratory parameters, including D-dimer and fibrinogen. Management of coagulopathy in COVID-19 patients is like that of critically ill patients, including thromboprophylaxis. Coagulopathy is a poor prognostic factor, and optimum strategies should be developed for early diagnosis, prevention, and prompt treatment of VTE in COVID-19 patients. Thrombosis prophylaxis with low molecular weight heparin (LMWH) has shown beneficial results in preventing coagulopathy a reducing risk of mortality due to thrombotic events. We will discuss VTE in COVID-19 patients highlighting the role of D-dimer, fibrinogen, and interleukin-6 (IL-6).
2019年12月下旬,新型冠状病毒肺炎(COVID-19)在中国南方海鲜批发市场西区出现,并被世界卫生组织(WHO)宣布为全球大流行疾病。感染严重急性呼吸综合征冠状病毒(SARS-CoV-2)会出现咳嗽、发热和乏力等上呼吸道症状。同时,在疾病后期,重症COVID-19患者会出现急性呼吸窘迫综合征(ARDS)、静脉血栓栓塞症(VTE)以及由细胞因子风暴和凝血亢进引发的多器官功能衰竭。血栓形成事件的主要表现包括深静脉血栓形成(DVT)、弥散性血管内凝血(DIC)和肺栓塞(PE)。COVID-19患者最初的凝血病表现为纤维蛋白降解产物升高,尤其是D-二聚体。相比之下,后期表现则显示凝血酶原时间(PT)和活化部分凝血活酶时间(aPTT)延长、血小板和纤维蛋白原水平升高。通过定期筛查包括D-二聚体和纤维蛋白原在内的实验室参数来诊断和监测疾病进展。COVID-19患者凝血病的管理与重症患者相似,包括血栓预防。凝血病是一个不良预后因素,应制定最佳策略用于COVID-19患者VTE的早期诊断、预防和及时治疗。低分子量肝素(LMWH)进行血栓预防已显示出在预防凝血病和降低血栓形成事件导致的死亡风险方面的有益效果。我们将讨论COVID-19患者中的VTE,重点强调D-二聚体、纤维蛋白原和白细胞介素-6(IL-6)的作用。