Department of Health Sciences, Hull York Medical School, University of York, York, UK.
Human Development and Health, Faculty of Medicine, University of Southampton, Southampton, UK.
Brain Behav. 2021 Feb;11(2):e01981. doi: 10.1002/brb3.1981. Epub 2020 Dec 4.
To provide an estimate of the effect of interventions on comorbid depressive disorder (MDD) or subthreshold depression in type 1 and type 2 diabetes.
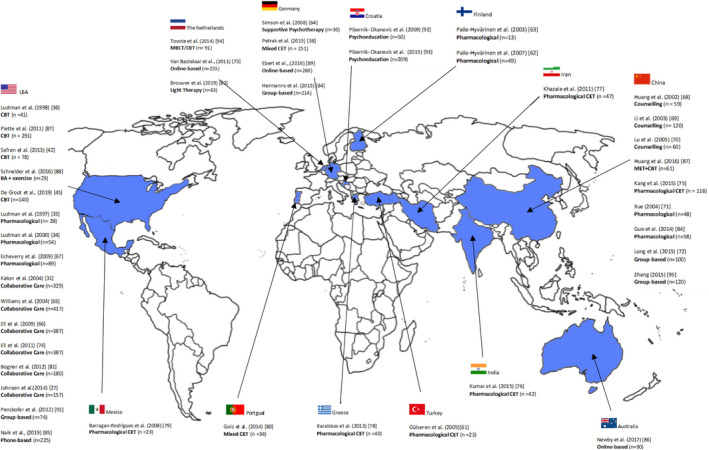
Systematic review and meta-analysis. We searched PubMed, PsycINFO, Embase, and the Cochrane Library for randomized controlled trials evaluating the outcome of depression treatments in diabetes and comorbid MDD or subthreshold symptoms published before August 2019 compared to care as usual (CAU), placebo, waiting list (WL), or active comparator treatment as in a comparative effectiveness trial (CET). Primary outcomes were depressive symptom severity and glycemic control. Cohen's d is reported.
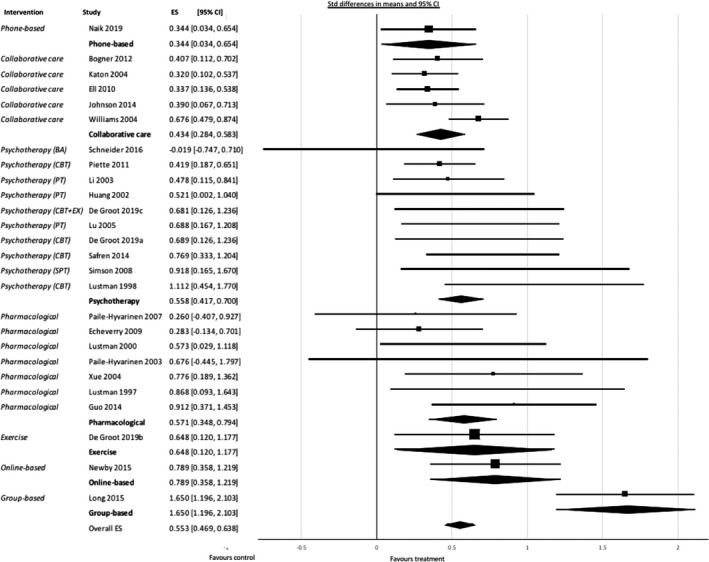
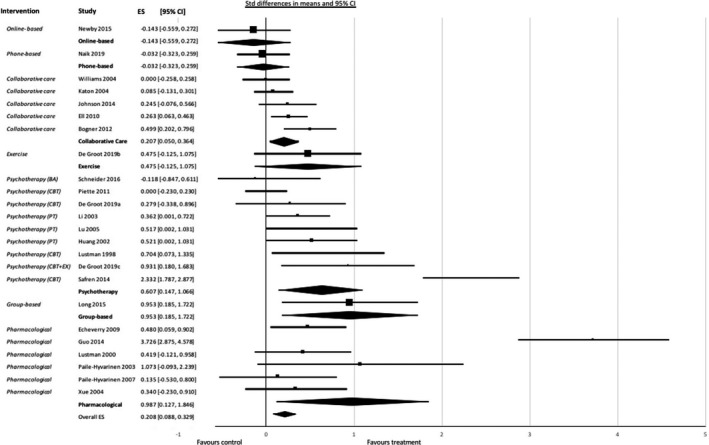
Forty-three randomized controlled trials (RCTs) were selected, and 32 RCTs comprising 3,543 patients were included in the meta-analysis. Our meta-analysis showed that, compared to CAU, placebo or WL, all interventions showed a significant effect on combined outcome 0,485 (95% CI 0.360; 0.609). All interventions showed a significant effect on depression. Pharmacological treatment, group therapy, psychotherapy, and collaborative care had a significant effect on glycemic control. High baseline depression score was associated with a greater reduction in HbA c and depressive outcome. High baseline HbA c was associated with a greater reduction in HbA c.
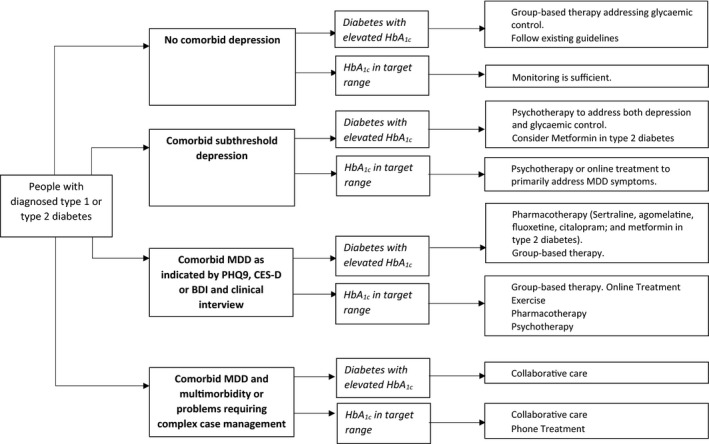
All treatments are effective for comorbid depression in type 1 diabetes and type 2 diabetes. Over the last decade, new interventions with large effect sizes have been introduced, such as group-based therapy, online treatment, and exercise. Although all interventions were effective for depression, not all treatments were effective for glycemic control. Effective interventions in comorbid depressive disorder may not be as effective in comorbid subthreshold depression. Baseline depression and HbA c scores modify the treatment effect. Based on the findings, we provide guidance for treatment depending on patient profile and desired outcome, and discuss possible avenues for further research.
评估干预措施对 1 型和 2 型糖尿病合并抑郁障碍(MDD)或亚临床抑郁的疗效。
系统评价和荟萃分析。我们检索了 PubMed、PsycINFO、Embase 和 Cochrane 图书馆,以寻找评估糖尿病和合并 MDD 或亚临床症状的抑郁治疗结果的随机对照试验,这些试验的研究结果发表于 2019 年 8 月之前,与常规治疗(CAU)、安慰剂、等待名单(WL)或作为比较有效性试验(CET)的活性对照治疗相比。主要结局是抑郁症状严重程度和血糖控制。报告 Cohen's d。
共纳入 43 项随机对照试验(RCT),其中 32 项 RCT 共纳入 3543 例患者,纳入荟萃分析。我们的荟萃分析表明,与 CAU、安慰剂或 WL 相比,所有干预措施对联合结局的影响均具有统计学意义(0.485,95%CI 0.360;0.609)。所有干预措施对抑郁均有显著疗效。药物治疗、团体治疗、心理治疗和协作护理对血糖控制有显著效果。高基线抑郁评分与 HbA c 和抑郁结局的显著降低相关。高基线 HbA c 与 HbA c 的显著降低相关。
所有治疗方法对 1 型和 2 型糖尿病合并抑郁障碍均有效。在过去十年中,引入了一些具有较大效果量的新干预措施,如基于团体的治疗、在线治疗和运动。尽管所有干预措施对抑郁均有效,但并非所有治疗方法对血糖控制均有效。在合并亚临床抑郁的情况下,对合并抑郁障碍有效的干预措施可能对亚临床抑郁的疗效并不显著。基线抑郁和 HbA c 评分会影响治疗效果。根据这些发现,我们根据患者特征和预期结果为治疗提供指导,并讨论了进一步研究的可能途径。