Keck School of Medicine, University of Southern California, Los Angeles, CA 90033, United States of America.
Keck School of Medicine, University of Southern California, Los Angeles, CA 90033, United States of America; Department of Integrative Anatomical Sciences, University of Southern California, Los Angeles, CA 90033, United States of America.
Semin Nucl Med. 2021 Jul;51(4):312-320. doi: 10.1053/j.semnuclmed.2020.11.003. Epub 2020 Nov 30.
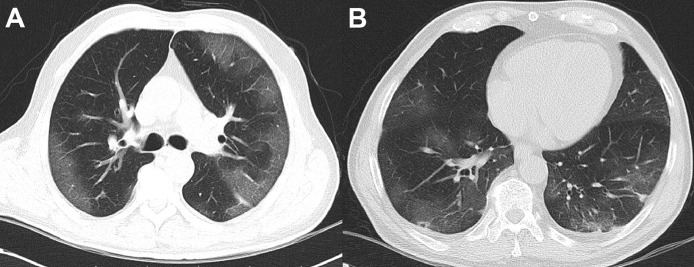
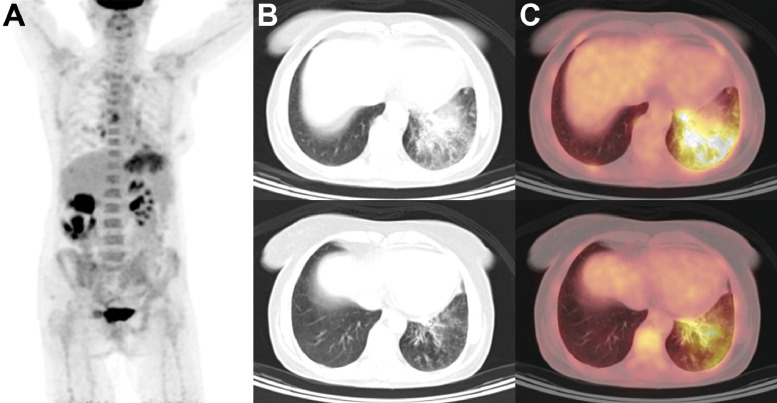
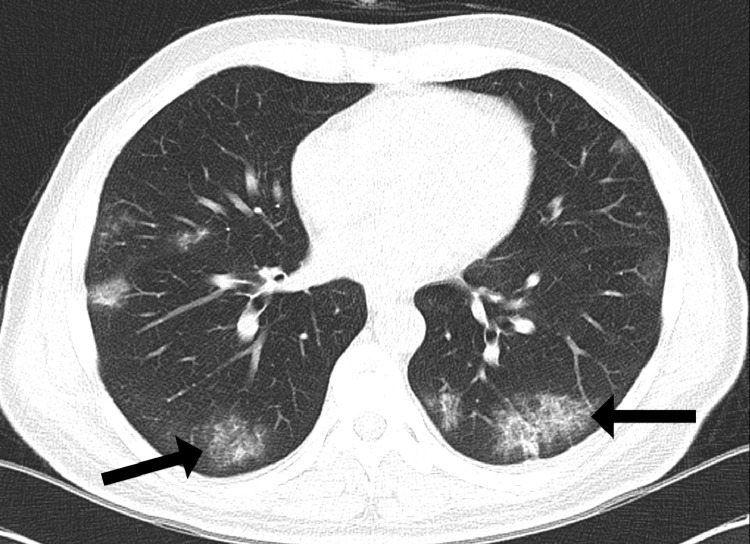
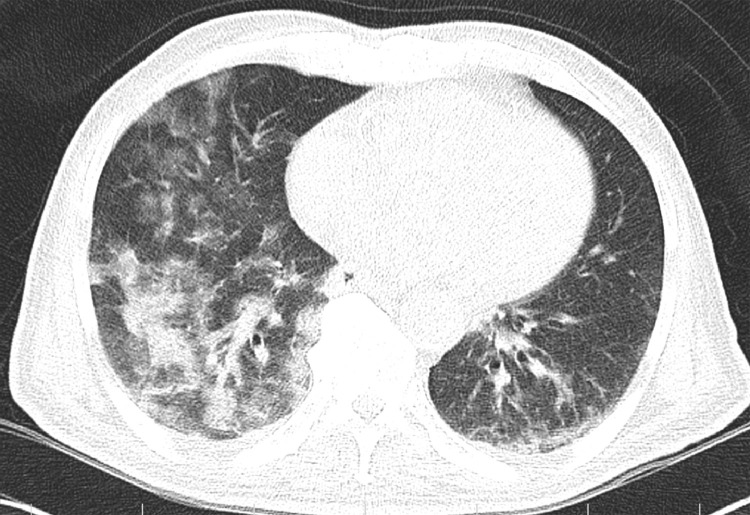
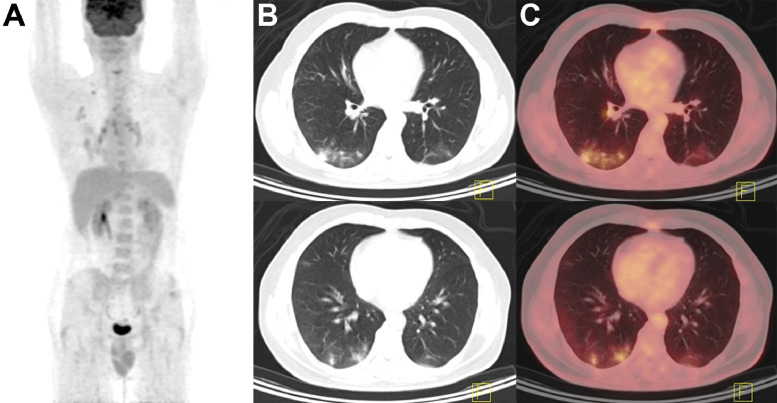
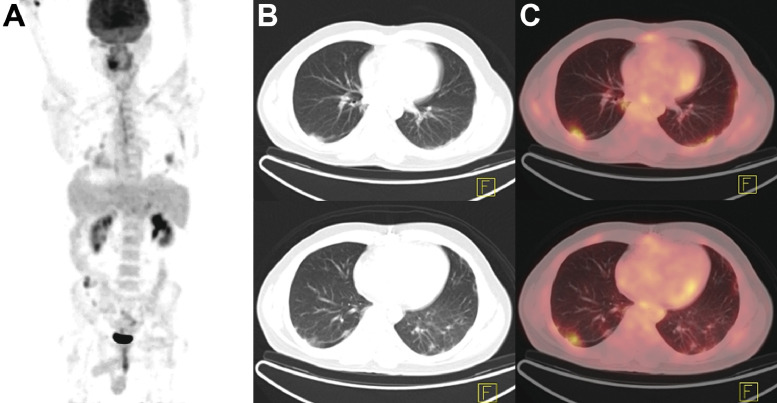
Soon after reports of a novel coronavirus capable of causing severe pneumonia surfaced in late 2019, expeditious global spread of the Severe Acute Respiratory Distress Syndrome Coronavirus 2 (SARS-CoV-2) forced the World Health Organization to declare an international state of emergency. Although best known for causing symptoms of upper respiratory tract infection in mild cases and fulminant pneumonia in severe disease, Coronavirus Disease 2019 (COVID-19) has also been associated with gastrointestinal, neurologic, cardiac, and hematologic presentations. Despite concerns over poor specificity and undue radiation exposure, chest imaging nonetheless remains central to the initial diagnosis and monitoring of COVID-19 progression, as well as to the evaluation of complications. Classic features on chest CT include ground-glass and reticular opacities with or without superimposed consolidations, frequently presenting in a bilateral, peripheral, and posterior distribution. More recently, studies conducted with MRI have shown excellent concordance with chest CT in visualizing typical features of COVID-19 pneumonia. For patients in whom exposure to ionizing radiation should be avoided, particularly pregnant patients and children, pulmonary MRI may represent a suitable alternative to chest CT. Although PET imaging is not typically considered among first-line investigative modalities for the diagnosis of lower respiratory tract infections, numerous reports have noted incidental localization of radiotracer in parenchymal regions of COVID-19-associated pulmonary lesions. These findings are consistent with data from Middle East Respiratory Syndrome-CoV cohorts which suggested an ability for F-FDG PET to detect subclinical infection and lymphadenitis in subjects without overt clinical signs of infection. Though highly sensitive, use of PET/CT for primary detection of COVID-19 is constrained by poor specificity, as well as considerations of cost, radiation burden, and prolonged exposure times for imaging staff. Even still, decontamination of scanner bays is a time-consuming process, and proper ventilation of scanner suites may additionally require up to an hour of downtime to allow for sufficient air exchange. Yet, in patients who require nuclear medicine investigations for other clinical indications, PET imaging may yield the earliest detection of nascent infection in otherwise asymptomatic individuals. Especially for patients with concomitant malignancies and other states of immunocompromise, prompt recognition of infection and early initiation of supportive care is crucial to maximizing outcomes and improving survivability.
2019 年末,一种新型冠状病毒能够引起严重肺炎的报告出现后不久,严重急性呼吸综合征冠状病毒 2(SARS-CoV-2)的迅速在全球传播,迫使世界卫生组织宣布进入国际紧急状态。尽管冠状病毒病 2019(COVID-19)最常引起轻度病例的上呼吸道感染症状和严重疾病的暴发性肺炎,但也与胃肠道、神经、心脏和血液学表现有关。尽管人们担心特异性差和过度辐射暴露,但胸部成像仍然是 COVID-19 初始诊断和监测进展以及评估并发症的核心。胸部 CT 的典型特征包括磨玻璃和网状混浊,伴有或不伴有叠加的实变,常呈双侧、外周和后分布。最近,使用 MRI 进行的研究表明,在可视化 COVID-19 肺炎的典型特征方面,与胸部 CT 具有极好的一致性。对于应避免接触电离辐射的患者,特别是孕妇和儿童,肺部 MRI 可能是胸部 CT 的合适替代方法。虽然 PET 成像通常不被认为是诊断下呼吸道感染的一线调查方式之一,但许多报告指出放射性示踪剂在 COVID-19 相关肺病变的实质区域的偶然定位。这些发现与中东呼吸综合征-CoV 队列的数据一致,表明 F-FDG PET 能够检测无明显临床感染迹象的亚临床感染和淋巴结炎。尽管高度敏感,但由于特异性差,以及成本、辐射负担和成像人员暴露时间延长等考虑因素,PET/CT 用于 COVID-19 的初始检测受到限制。即便如此,扫描仪舱的去污仍然是一个耗时的过程,扫描仪套件的适当通风可能还需要长达一小时的停机时间,以允许足够的空气交换。然而,对于需要进行核医学检查的其他临床指征的患者,PET 成像可能会在其他无症状个体中最早发现新生感染。特别是对于伴有合并症和其他免疫功能低下状态的患者,及时识别感染并尽早开始支持性护理对于最大限度地提高结果和提高生存率至关重要。