EPI-PHARE Scientific Interest Group in Epidemiology of Health Products from the French National Agency for the Safety of Medicines and Health Products, Saint-Denis, France and the French National Health Insurance, Paris, France (L.S., J.B., B.B., C.V., J.D., F.C., L.P., P.H., E.S., A.W., R.D.-S., M.Z.).
Epidemiology in Dermatology and Evaluation of Therapeutics Research Unit, University Paris-Est Créteil (E.S.).
Hypertension. 2021 Mar 3;77(3):833-842. doi: 10.1161/HYPERTENSIONAHA.120.16314. Epub 2021 Jan 11.
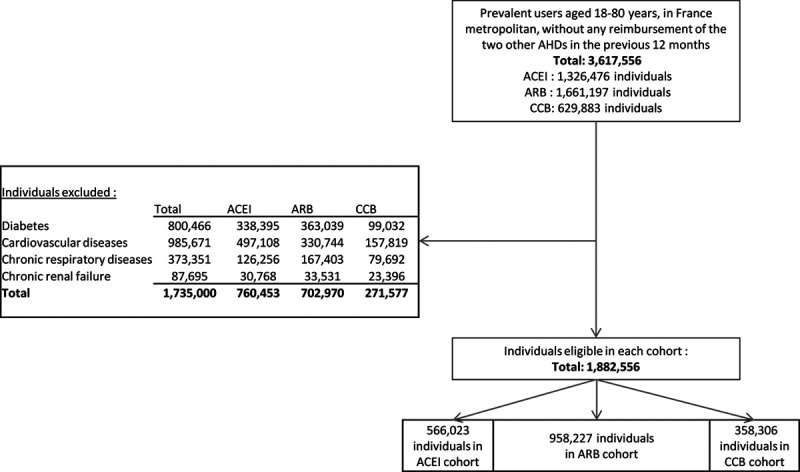
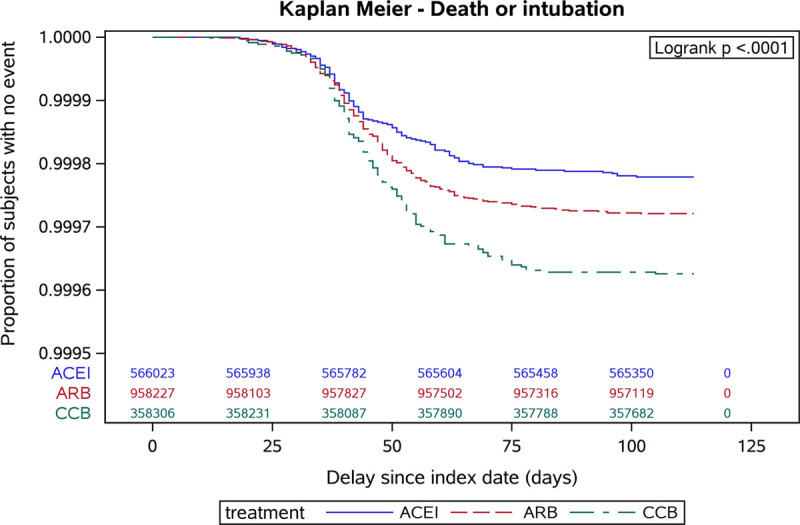
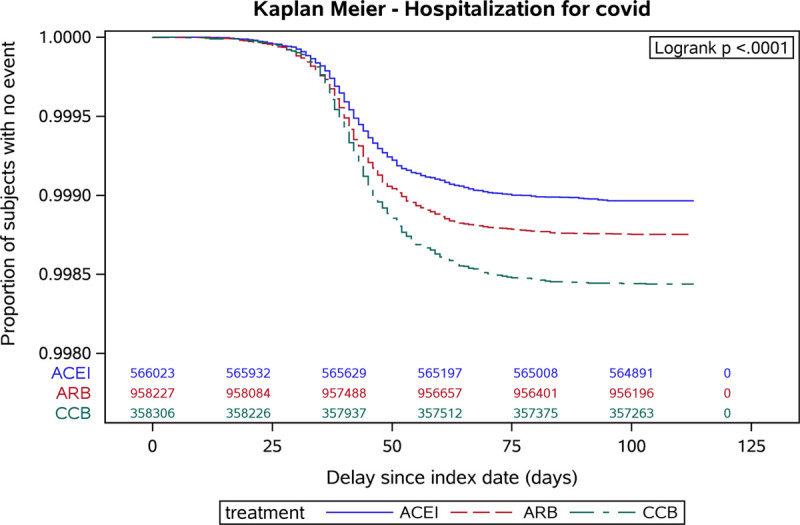
After initially hypothesizing a positive relationship between use of renin-angiotensin-aldosterone system inhibitors and risk of coronavirus disease 2019 (COVID-19), more recent evidence suggests negative associations. We examined whether COVID-19 risk differs according to antihypertensive drug class in patients treated by ACE (angiotensin-converting enzyme) inhibitors and angiotensin receptor blockers (ARBs) compared with calcium channel blockers (CCBs). Three exclusive cohorts of prevalent ACE inhibitors, ARB and CCB users, aged 18 to 80 years, from the French National Health Insurance databases were followed from February 15, 2020 to June 7, 2020. We excluded patients with a history of diabetes, known cardiovascular disease, chronic renal failure, or chronic respiratory disease during the previous 5 years, to only consider patients treated for uncomplicated hypertension and to limit indication bias. The primary end point was time to hospitalization for COVID-19. The secondary end point was time to intubation/death during a hospital stay for COVID-19. In a population of almost 2 million hypertensive patients (ACE inhibitors: 566 023; ARB: 958 227; CCB: 358 306) followed for 16 weeks, 2338 were hospitalized and 526 died or were intubated for COVID-19. ACE inhibitors and ARBs were associated with a lower risk of COVID-19 hospitalization compared with CCBs (hazard ratio, 0.74 [95% CI, 0.65-0.83] and 0.84 [0.76-0.93], respectively) and a lower risk of intubation/death. Risks were slightly lower for ACE inhibitor users than for ARB users. This large observational study may suggest a lower COVID-19 risk in hypertensive patients treated over a long period with ACE inhibitors or ARBs compared with CCBs. These results, if confirmed, tend to contradict previous hypotheses and raise new hypotheses.
最初假设血管紧张素转换酶抑制剂和血管紧张素受体阻滞剂(ARB)的使用与 2019 年冠状病毒病(COVID-19)风险呈正相关,但最近的证据表明存在负相关。我们研究了与钙通道阻滞剂(CCB)相比,接受 ACE(血管紧张素转换酶)抑制剂和 ARB 治疗的患者,COVID-19 风险是否因抗高血压药物类别而异。从 2020 年 2 月 15 日至 2020 年 6 月 7 日,从法国国家健康保险数据库中随访了三个独特的 ACE 抑制剂、ARB 和 CCB 现有使用者队列,年龄在 18 至 80 岁之间。我们排除了过去 5 年内患有糖尿病、已知心血管疾病、慢性肾衰竭或慢性呼吸道疾病的患者,仅考虑接受单纯高血压治疗的患者,并限制适应症偏倚。主要终点是因 COVID-19 住院的时间。次要终点是 COVID-19 住院期间插管/死亡的时间。在近 200 万高血压患者(ACE 抑制剂:566023 人;ARB:958227 人;CCB:358306 人)中,随访了 16 周,有 2338 人因 COVID-19 住院,526 人死亡或插管。与 CCB 相比,ACE 抑制剂和 ARB 与 COVID-19 住院风险降低相关(风险比分别为 0.74[95%CI,0.65-0.83]和 0.84[0.76-0.93]),插管/死亡风险也降低。ACE 抑制剂使用者的风险略低于 ARB 使用者。这项大型观察性研究可能表明,与 CCB 相比,长期接受 ACE 抑制剂或 ARB 治疗的高血压患者 COVID-19 风险较低。如果这些结果得到证实,往往与之前的假设相矛盾,并提出新的假设。