Grasselli Giacomo, Giani Marco, Scaravilli Vittorio, Fumagalli Benedetta, Mariani Carminia, Redaelli Sara, Lucchini Alberto, Zanella Alberto, Patroniti Nicolò, Pesenti Antonio, Foti Giuseppe
Dipartimento di Fisiopatologia Medico Chirurgica e dei Trapianti, Università degli Studi di Milano, Milan, Italy.
Dipartimento di Anestesia-Rianimazione e Emergenza Urgenza, Fondazione IRCCS Ca' Granda Ospedale Maggiore Policlinico, Milan, Italy.
Crit Care Explor. 2021 Jan 8;3(1):e0310. doi: 10.1097/CCE.0000000000000310. eCollection 2021 Jan.
Patients on extracorporeal support for severe acute respiratory distress syndrome may require a prolonged period of deep sedation. In these patients, volatile sedation may represent a valid alternative to IV drugs. The aim of our study was to describe the feasibility of volatile sedation in a large cohort of acute respiratory distress syndrome patients undergoing venovenous extracorporeal membrane oxygenation and ultraprotective ventilation.
Retrospective monocentric study.
Adult ICU, ASST Monza, Italy.
Adult patients who underwent volatile sedation with isoflurane during venovenous extracorporeal membrane oxygenation between 2009 and 2019.
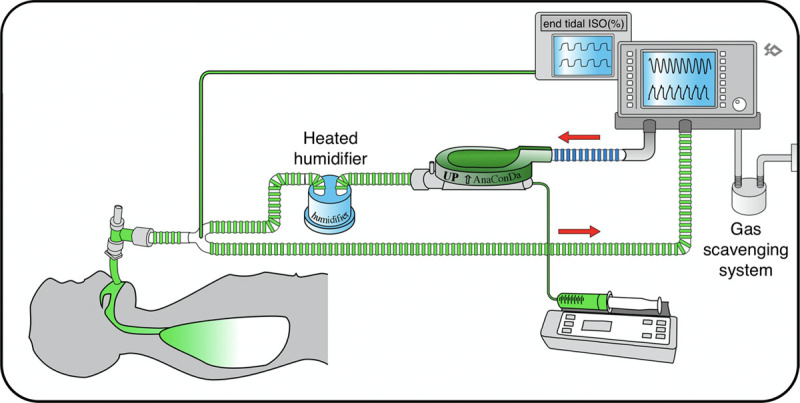
Isoflurane was delivered via the AnaConDa system. The sedation level, hemodynamics, and laboratory tests were compared between the volatile sedation phase and the IV sedation phases before and after the isoflurane sedation period.
About 74 patients (50 yr [43-56 yr]) were included. Median duration of venovenous extracorporeal membrane oxygenation support was 22 days (14-51 d). Volatile sedation started on day 3 (2-6) of extracorporeal membrane oxygenation support, and its median duration was 7 days (4-13 d), ranging from 1 to 38 days. A total of 970 venovenous extracorporeal membrane oxygenation days were analyzed. During the volatile phase, the sedation level was slightly deeper (bispectral index 39 ± 6) compared with the IV phase before and after isoflurane (42 ± 8 and 43 ± 9, respectively, < 0.001). Requirements of fentanyl and remifentanyl were reduced during the volatile phase. Minor differences in hemodynamics were observed during volatile sedation: mean arterial pressure was lower (75 ± 13 vs 79 ± 14 and 80 ± 15; < 0.001), whereas cardiac output was higher (8.5 ± 1.9 vs 7.9 ± 1.8 and 8.0 ± 1.8; = 0.003). Aspartate aminotransferase levels were lower during the volatile sedation phases ( < 0.001), whereas alanine aminotransferase, triglycerides, and creatine phosphokinase were more altered during the IV sedation phase before isoflurane ( < 0.001).
Volatile sedation represents an alternative to IV agents to achieve long-term deep sedation in critically ill patients on extracorporeal membrane oxygenation undergoing ultraprotective ventilation.
接受体外支持治疗严重急性呼吸窘迫综合征的患者可能需要长时间深度镇静。对于这些患者,挥发性镇静剂可能是静脉用药的有效替代方案。我们研究的目的是描述在一大群接受静脉 - 静脉体外膜肺氧合和超保护性通气的急性呼吸窘迫综合征患者中使用挥发性镇静剂的可行性。
回顾性单中心研究。
意大利蒙扎ASST成人重症监护病房。
2009年至2019年间在静脉 - 静脉体外膜肺氧合期间接受异氟烷挥发性镇静的成年患者。
通过AnaConDa系统给予异氟烷。比较挥发性镇静阶段与异氟烷镇静期前后静脉镇静阶段的镇静水平、血流动力学和实验室检查结果。
纳入约74例患者(年龄50岁[43 - 56岁])。静脉 - 静脉体外膜肺氧合支持的中位持续时间为22天(14 - 51天)。挥发性镇静在体外膜肺氧合支持的第3天(2 - 6天)开始,中位持续时间为7天(4 - 13天),范围为1至38天。共分析了970个静脉 - 静脉体外膜肺氧合日。在挥发性阶段,镇静水平比异氟烷前后的静脉阶段略深(脑电双频指数39±6)(分别为42±8和43±9,P<0.001)。在挥发性阶段,芬太尼和瑞芬太尼的需求量减少。在挥发性镇静期间观察到血流动力学有微小差异:平均动脉压较低(75±13 vs 79±14和80±15;P<0.001),而心输出量较高(8.5±1.9 vs 7.9±1.8和8.0±1.8;P = 0.003)。在挥发性镇静阶段,天冬氨酸转氨酶水平较低(P<0.001),而异丙氨酸转氨酶、甘油三酯和肌酸磷酸激酶在异氟烷前的静脉镇静阶段变化更大(P<0.001)。
对于接受超保护性通气的体外膜肺氧合重症患者,挥发性镇静是实现长期深度镇静的静脉用药替代方案。