Centre for Experimental Medicine and Rheumatology, Queen Mary University of London, London, UK; Department of Rheumatology, Mile End Hospital, Barts Health NHS Trust, London, UK.
Department of Rheumatology, Cliniques Universitaires Saint-Luc, Brussels, Belgium; Institute of Experimental and Clinical Research, Université catholique de Louvain, Brussels, Belgium.
Lancet. 2021 Jan 23;397(10271):305-317. doi: 10.1016/S0140-6736(20)32341-2.
Although targeted biological treatments have transformed the outlook for patients with rheumatoid arthritis, 40% of patients show poor clinical response, which is mechanistically still unexplained. Because more than 50% of patients with rheumatoid arthritis have low or absent CD20 B cells-the target for rituximab-in the main disease tissue (joint synovium), we hypothesised that, in these patients, the IL-6 receptor inhibitor tocilizumab would be more effective. The aim of this trial was to compare the effect of tocilizumab with rituximab in patients with rheumatoid arthritis who had an inadequate response to anti-tumour necrosis factor (TNF) stratified for synovial B-cell status.
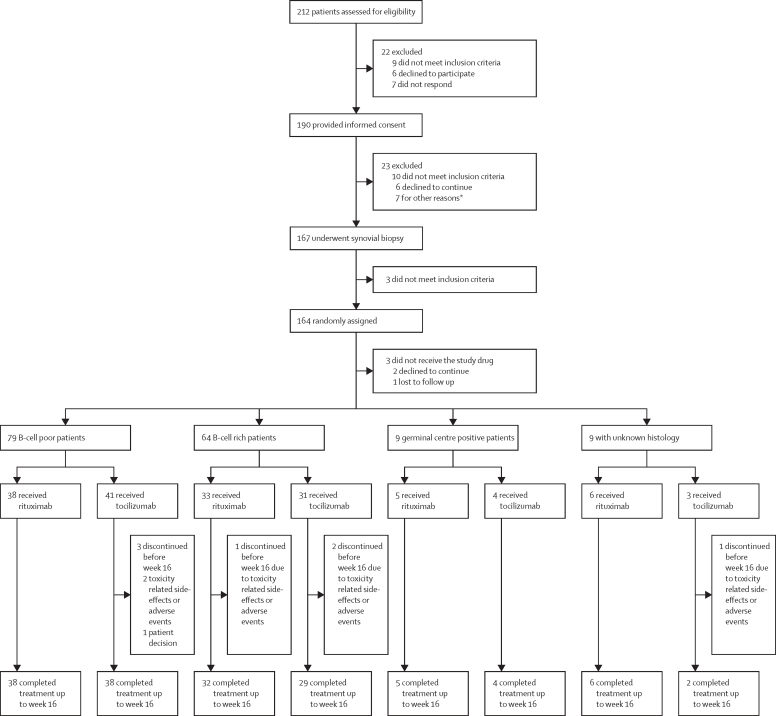
This study was a 48-week, biopsy-driven, multicentre, open-label, phase 4 randomised controlled trial (rituximab vs tocilizumab in anti-TNF inadequate responder patients with rheumatoid arthritis; R4RA) done in 19 centres across five European countries (the UK, Belgium, Italy, Portugal, and Spain). Patients aged 18 years or older who fulfilled the 2010 American College of Rheumatology and European League Against Rheumatism classification criteria for rheumatoid arthritis and were eligible for treatment with rituximab therapy according to UK National Institute for Health and Care Excellence guidelines were eligible for inclusion in the trial. To inform balanced stratification, following a baseline synovial biopsy, patients were classified histologically as B-cell poor or rich. Patients were then randomly assigned (1:1) centrally in block sizes of six and four to receive two 1000 mg rituximab infusions at an interval of 2 weeks (rituximab group) or 8 mg/kg tocilizumab infusions at 4-week intervals (tocilizumab group). To enhance the accuracy of the stratification of B-cell poor and B-cell rich patients, baseline synovial biopsies from all participants were subjected to RNA sequencing and reclassified by B-cell molecular signature. The study was powered to test the superiority of tocilizumab over rituximab in the B-cell poor population at 16 weeks. The primary endpoint was defined as a 50% improvement in Clinical Disease Activity Index (CDAI50%) from baseline. The trial is registered on the ISRCTN database, ISRCTN97443826, and EudraCT, 2012-002535-28.
Between Feb 28, 2013, and Jan 17, 2019, 164 patients were classified histologically and were randomly assigned to the rituximab group (83 [51%]) or the tocilizumab group (81 [49%]). In patients histologically classified as B-cell poor, there was no statistically significant difference in CDAI50% between the rituximab group (17 [45%] of 38 patients) and the tocilizumab group (23 [56%] of 41 patients; difference 11% [95% CI -11 to 33], p=0·31). However, in the synovial biopsies classified as B-cell poor with RNA sequencing the tocilizumab group had a significantly higher response rate compared with the rituximab group for CDAI50% (rituximab group 12 [36%] of 33 patients vs tocilizumab group 20 [63%] of 32 patients; difference 26% [2 to 50], p=0·035). Occurrence of adverse events (rituximab group 76 [70%] of 108 patients vs tocilizumab group 94 [80%] of 117 patients; difference 10% [-1 to 21) and serious adverse events (rituximab group 8 [7%] of 108 vs tocilizumab group 12 [10%] of 117; difference 3% [-5 to 10]) were not significantly different between treatment groups.
The results suggest that RNA sequencing-based stratification of rheumatoid arthritis synovial tissue showed stronger associations with clinical responses compared with histopathological classification. Additionally, for patients with low or absent B-cell lineage expression signature in synovial tissue tocilizumab is more effective than rituximab. Replication of the results and validation of the RNA sequencing-based classification in independent cohorts is required before making treatment recommendations for clinical practice.
Efficacy and Mechanism Evaluation programme from the UK National Institute for Health Research.
尽管靶向生物治疗已经改变了类风湿关节炎患者的前景,但仍有 40%的患者表现出较差的临床反应,其机制仍未得到解释。因为在主要疾病组织(关节滑膜)中,超过 50%的类风湿关节炎患者的 CD20 B 细胞(利妥昔单抗的靶标)数量较低或不存在,所以我们假设在这些患者中,白细胞介素-6 受体抑制剂托珠单抗的疗效会更好。本试验旨在比较托珠单抗与利妥昔单抗在抗肿瘤坏死因子(TNF)治疗反应不足的类风湿关节炎患者中的疗效,这些患者根据滑膜 B 细胞状态进行分层。
这是一项为期 48 周、基于活检、多中心、开放性、4 期随机对照试验(R4RA),在英国、比利时、意大利、葡萄牙和西班牙的 19 个中心进行。年龄在 18 岁或以上的患者,符合 2010 年美国风湿病学会和欧洲抗风湿病联盟的类风湿关节炎分类标准,并且根据英国国家卫生与保健优化研究所的指南有资格接受利妥昔单抗治疗的患者,都有资格入组本试验。为了进行均衡分层,在基线滑膜活检后,根据组织学将患者分为 B 细胞缺乏或丰富。然后患者被中央随机分配(1:1)至利妥昔单抗组(83 例[51%])或托珠单抗组(81 例[49%]),每组间隔 2 周接受两次 1000mg 利妥昔单抗输注,或每 4 周接受 8mg/kg 托珠单抗输注。为了提高 B 细胞缺乏和 B 细胞丰富患者分层的准确性,所有参与者的基线滑膜活检均进行 RNA 测序,并通过 B 细胞分子特征进行重新分类。该试验有足够的效力来检验托珠单抗在 16 周时优于利妥昔单抗在 B 细胞缺乏患者中的疗效。主要终点定义为从基线开始临床疾病活动指数(CDAI50%)改善 50%。该试验在 ISRCTN 数据库、ISRCTN97443826 和 EudraCT 上注册,注册号为 2012-002535-28。
2013 年 2 月 28 日至 2019 年 1 月 17 日期间,164 名患者进行了组织学分类,并随机分配至利妥昔单抗组(83 例[51%])或托珠单抗组(81 例[49%])。在组织学上被分类为 B 细胞缺乏的患者中,利妥昔单抗组(38 例中有 17 例[45%])和托珠单抗组(41 例中有 23 例[56%])的 CDAI50%之间没有统计学上的显著差异(差异 11%[-11 至 33],p=0.31)。然而,在 RNA 测序分类为 B 细胞缺乏的滑膜活检中,托珠单抗组的 CDAI50%反应率明显高于利妥昔单抗组(利妥昔单抗组 33 例中有 12 例[36%],托珠单抗组 32 例中有 20 例[63%];差异 26%[2 至 50],p=0.035)。不良事件的发生率(利妥昔单抗组 108 例中有 76 例[70%],托珠单抗组 117 例中有 94 例[80%];差异 10%[-1 至 21])和严重不良事件的发生率(利妥昔单抗组 108 例中有 8 例[7%],托珠单抗组 117 例中有 12 例[10%];差异 3%[-5 至 10])在治疗组之间没有显著差异。
结果表明,基于 RNA 测序的类风湿关节炎滑膜组织分层与临床反应的相关性比组织病理学分类更强。此外,对于滑膜组织中 B 细胞谱系表达特征低或不存在的患者,托珠单抗比利妥昔单抗更有效。在独立队列中复制这些结果并验证 RNA 测序分类,然后才能为临床实践提出治疗建议。
英国国家卫生与保健优化研究所的疗效和机制评估计划。