Department of Neurology, Xijing Hospital, Fourth Military Medical University, Xi'an, China.
Int J Med Sci. 2021 Jan 9;18(5):1167-1178. doi: 10.7150/ijms.52752. eCollection 2021.
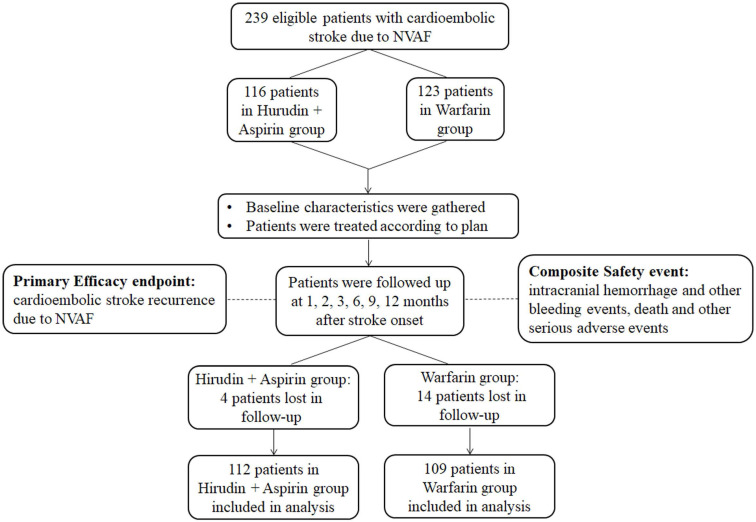
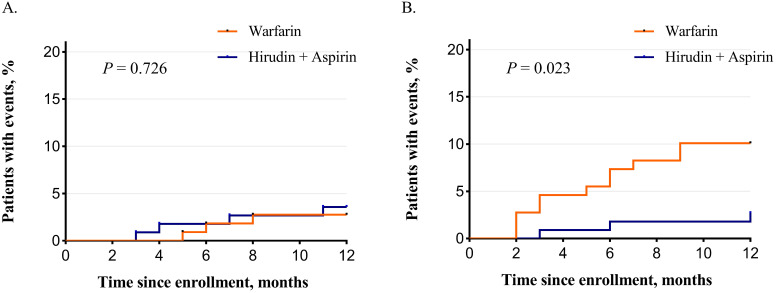
To investigate the efficacy and safety of hirudin plus aspirin therapy compared with warfarin in the secondary prevention of cardioembolic stroke due to nonvalvular atrial fibrillation (NVAF). Patients with cardioembolic stroke due to NVAF were prospectively enrolled from 18 collaborating hospitals from Dec 2011 to June 2015. Fourteen days after stroke onset, eligible patients were assigned to the hirudin plus aspirin group (natural hirudin prescribed as the traditional Chinese medicine Maixuekang capsule, 0.75 g, three times daily, combined with aspirin 100 mg, once daily) or the warfarin group (dose-adjusted warfarin targeting international normalized ratio (INR) 2-3, with an initial daily dose of 1.25 mg). Patients were followed up at 1, 2, 3, 6, 9, and 12 months after stroke onset. Time in therapeutic range (TTR) was calculated according to Rosendaal methodology to evaluate the quality of INR management in the warfarin group. The primary efficacy endpoint was the recurrence of stroke within 12 months after stroke onset. Safety was assessed as the occurrence of the composite event "intracranial hemorrhage and other bleeding events, death, and other serious adverse events". The Cox proportional hazard model and Kaplan-Meier curve were used to analyze the efficacy and safety events. A total of 221 patients entered final analysis with 112 patients in the hirudin plus aspirin group and 109 in the warfarin group. Over the whole duration of our study, TTR for patients taking warfarin was 66.5 % ± 21.5%. A significant difference was not observed in the recurrence of stroke between the two groups (3.57% vs. 2.75%; = 0.728). The occurrence of safety events was significantly lower in the hirudin plus aspirin group (2.68% vs.10.09%; = 0.024). The risk for efficacy event was similar between the two groups (hazard ratio (HR), 1.30; 95% confidence interval (CI), 0.29-5.80). The safety risk was significantly lower in the hirudin plus aspirin group (HR, 0.27; 95% CI, 0.07-0.95). Kaplan-Meier analysis revealed significant difference in the temporal distribution in safety events ( = 0.023) but not in stroke recurrence ( = 0.726). Significant difference in efficacy was not detected between warfarin group and hirudin plus aspirin group. Compared with warfarin, hirudin plus aspirin therapy had lower safety risk in the secondary prevention of cardioembolic stroke due to NVAF.
为了研究与华法林相比,水蛭素加阿司匹林治疗在非瓣膜性心房颤动(NVAF)引起的心源性栓塞性中风二级预防中的疗效和安全性。2011 年 12 月至 2015 年 6 月,从 18 家合作医院前瞻性招募心源性栓塞性中风患者。中风发作后 14 天,符合条件的患者被分配到水蛭素加阿司匹林组(天然水蛭素按中药脉血康胶囊规定,每次 0.75 克,每日 3 次,联合阿司匹林 100 毫克,每日 1 次)或华法林组(调整剂量的华法林,目标国际标准化比值(INR)为 2-3,初始日剂量为 1.25 毫克)。患者在中风发作后 1、2、3、6、9 和 12 个月进行随访。根据 Rosendaal 方法计算治疗时间范围(TTR),以评估华法林组 INR 管理的质量。主要疗效终点为中风发作后 12 个月内中风复发。安全性评估为“颅内出血和其他出血事件、死亡和其他严重不良事件”的复合事件发生情况。Cox 比例风险模型和 Kaplan-Meier 曲线用于分析疗效和安全性事件。共有 221 例患者进入最终分析,其中水蛭素加阿司匹林组 112 例,华法林组 109 例。在整个研究期间,服用华法林的患者 TTR 为 66.5%±21.5%。两组中风复发率无显著差异(3.57%比 2.75%;=0.728)。水蛭素加阿司匹林组的安全性事件发生率明显较低(2.68%比 10.09%;=0.024)。两组疗效事件风险相似(危险比(HR),1.30;95%置信区间(CI),0.29-5.80)。水蛭素加阿司匹林组安全性风险显著降低(HR,0.27;95%CI,0.07-0.95)。Kaplan-Meier 分析显示,安全性事件的时间分布存在显著差异(=0.023),但中风复发无显著差异(=0.726)。华法林组与水蛭素加阿司匹林组之间未检测到疗效差异。与华法林相比,水蛭素加阿司匹林治疗在非瓣膜性心房颤动引起的心源性栓塞性中风二级预防中具有较低的安全性风险。