Key Laboratory of OptoElectronic Science and Technology for Medicine of Ministry of Education, Fujian Provincial Key Laboratory of Photonics Technology, Fujian Normal University, Fuzhou, China.
Breast Surgery Ward, Department of General Surgery, Fujian Medical University Union Hospital, Fuzhou, China.
Theranostics. 2021 Jan 1;11(7):3229-3243. doi: 10.7150/thno.55921. eCollection 2021.
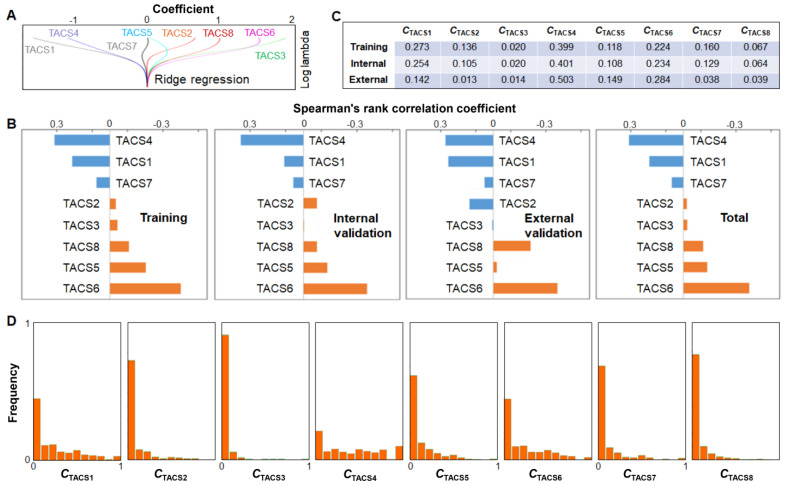
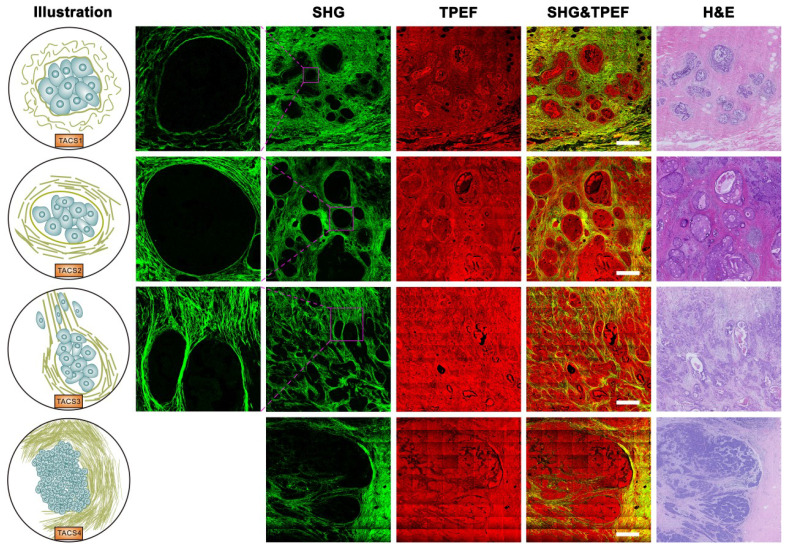
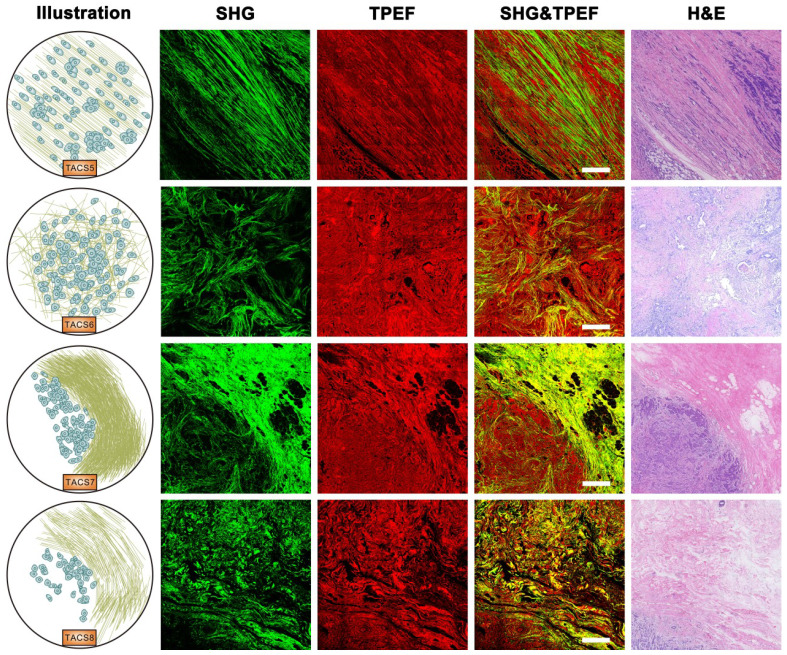
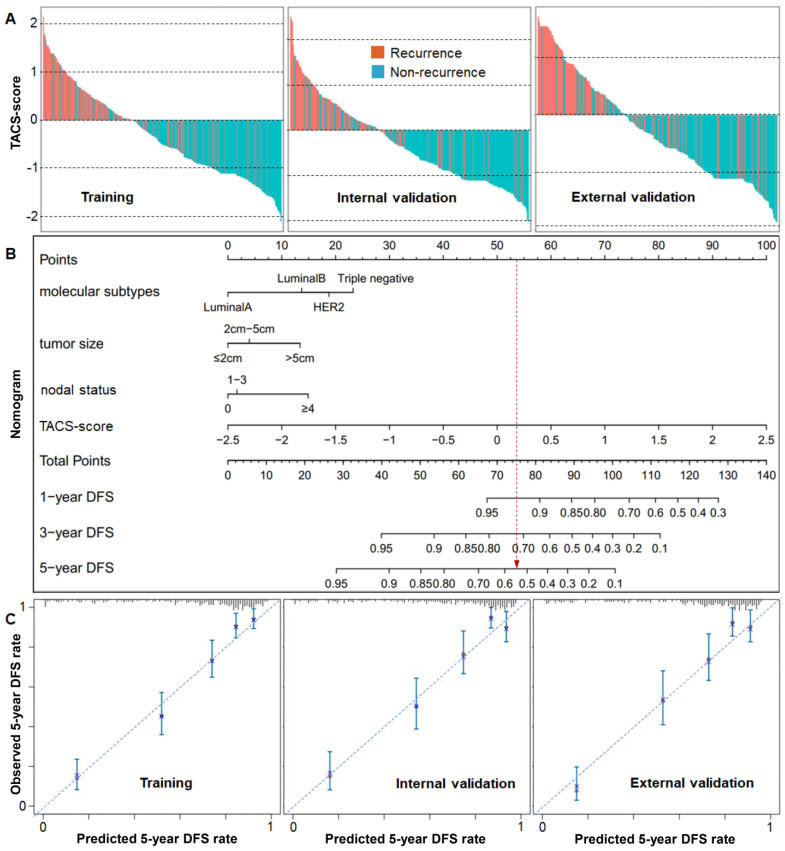
The notion of personalized medicine demands proper prognostic biomarkers to guide the optimal therapy for an invasive breast cancer patient. However, various risk prediction models based on conventional clinicopathological factors and emergent molecular assays have been frequently limited by either a low strength of prognosis or restricted applicability to specific types of patients. Therefore, there is a critical need to develop a strong and general prognosticator. We observed five large-scale tumor-associated collagen signatures (TACS4-8) obtained by multiphoton microscopy at the invasion front of the breast primary tumor, which contrasted with the three tumor-associated collagen signatures (TACS1-3) discovered by Keely and coworkers at a smaller scale. Highly concordant TACS1-8 classifications were obtained by three independent observers. Using the ridge regression analysis, we obtained a TACS-score for each patient based on the combined TACS1-8 and established a risk prediction model based on the TACS-score. In a blind fashion, consistent retrospective prognosis was obtained from 995 breast cancer patients in both a training cohort (= 431) and an internal validation cohort ( = 300) collected from one clinical center, and in an external validation cohort ( = 264) collected from a different clinical center. Results: TACS1-8 model alone competed favorably with all reported models in predicting disease-free survival (AUC: 0.838, [0.800-0.872]; 0.827, [0.779-0.868]; 0.807, [0.754-0.853] in the three cohorts) and stratifying low- and high-risk patients (HR 7.032, [4.869-10.158]; 6.846, [4.370-10.726], 4.423, [2.917-6.708]). The combination of these factors with the TACS-score into a nomogram model further improved the prognosis (AUC: 0.865, [0.829-0.896]; 0.861, [0.816-0.898]; 0.854, [0.805-0.894]; HR 7.882, [5.487-11.323]; 9.176, [5.683-14.816], and 5.548, [3.705-8.307]). The nomogram identified 72 of 357 (~20%) patients with unsuccessful 5-year disease-free survival that might have been undertreated postoperatively. Conclusions: The risk prediction model based on TACS1-8 considerably outperforms the contextual clinical model and may thus convince pathologists to pursue a TACS-based breast cancer prognosis. Our methodology identifies a significant portion of patients susceptible to undertreatment (high-risk patients), in contrast to the multigene assays that often strive to mitigate overtreatment. The compatibility of our methodology with standard histology using traditional (non-tissue-microarray) formalin-fixed paraffin-embedded (FFPE) tissue sections could simplify subsequent clinical translation.
个性化医学的概念需要适当的预后生物标志物来指导浸润性乳腺癌患者的最佳治疗。然而,基于常规临床病理因素和新兴分子检测的各种风险预测模型,要么预后强度较低,要么适用范围仅限于特定类型的患者。因此,迫切需要开发一种强大且通用的预后标志物。
我们观察了五个通过多光子显微镜在乳腺原发性肿瘤侵袭前沿获得的大型肿瘤相关胶原特征(TACS4-8),与 Keely 及其同事在较小规模发现的三个肿瘤相关胶原特征(TACS1-3)形成对比。三位独立观察者获得了高度一致的 TACS1-8 分类。使用岭回归分析,我们根据组合的 TACS1-8 为每位患者获得了 TACS 评分,并基于 TACS 评分建立了风险预测模型。以盲法从一个临床中心收集的 995 名乳腺癌患者的训练队列(= 431)和内部验证队列(= 300)以及来自不同临床中心的外部验证队列(= 264)中获得了一致的回顾性预后。结果:TACS1-8 模型单独预测无病生存(AUC:0.838,[0.800-0.872];0.827,[0.779-0.868];0.807,[0.754-0.853])和分层低风险和高风险患者(HR 7.032,[4.869-10.158];6.846,[4.370-10.726],4.423,[2.917-6.708])的表现优于所有报告的模型。这些因素与 TACS 评分相结合纳入列线图模型进一步改善了预后(AUC:0.865,[0.829-0.896];0.861,[0.816-0.898];0.854,[0.805-0.894];HR 7.882,[5.487-11.323];9.176,[5.683-14.816],和 5.548,[3.705-8.307])。列线图确定了 357 名患者中有 72 名(~20%)的 5 年无病生存不成功,这些患者可能术后治疗不足。结论:基于 TACS1-8 的风险预测模型显著优于上下文临床模型,因此可能说服病理学家进行基于 TACS 的乳腺癌预后。我们的方法确定了很大一部分易治疗不足的患者(高危患者),与经常努力减轻过度治疗的多基因检测形成对比。我们的方法与使用传统(非组织微阵列)福尔马林固定石蜡包埋(FFPE)组织切片的标准组织学的兼容性可以简化后续的临床转化。