Stroke Diagnostic and Monitoring Division, AtheroPoint™, Roseville, CA, USA.
Advanced Knowledge Engineering Centre, GBTI, Roseville, CA, USA; Department of Computer Science Engineering, PSIT, Kanpur, India.
Comput Biol Med. 2021 Mar;130:104210. doi: 10.1016/j.compbiomed.2021.104210. Epub 2021 Jan 18.
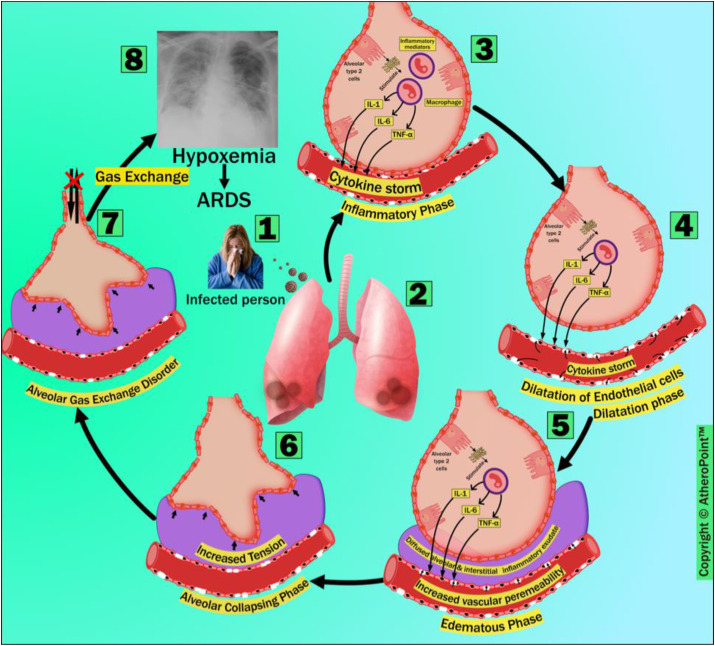
COVID-19 has infected 77.4 million people worldwide and has caused 1.7 million fatalities as of December 21, 2020. The primary cause of death due to COVID-19 is Acute Respiratory Distress Syndrome (ARDS). According to the World Health Organization (WHO), people who are at least 60 years old or have comorbidities that have primarily been targeted are at the highest risk from SARS-CoV-2. Medical imaging provides a non-invasive, touch-free, and relatively safer alternative tool for diagnosis during the current ongoing pandemic. Artificial intelligence (AI) scientists are developing several intelligent computer-aided diagnosis (CAD) tools in multiple imaging modalities, i.e., lung computed tomography (CT), chest X-rays, and lung ultrasounds. These AI tools assist the pulmonary and critical care clinicians through (a) faster detection of the presence of a virus, (b) classifying pneumonia types, and (c) measuring the severity of viral damage in COVID-19-infected patients. Thus, it is of the utmost importance to fully understand the requirements of for a fast and successful, and timely lung scans analysis. This narrative review first presents the pathological layout of the lungs in the COVID-19 scenario, followed by understanding and then explains the comorbid statistical distributions in the ARDS framework. The novelty of this review is the approach to classifying the AI models as per the by school of thought (SoTs), exhibiting based on segregation of techniques and their characteristics. The study also discusses the identification of AI models and its extension from non-ARDS lungs (pre-COVID-19) to ARDS lungs (post-COVID-19). Furthermore, it also presents AI workflow considerations of for medical imaging modalities in the COVID-19 framework. Finally, clinical AI design considerations will be discussed. We conclude that the design of the current existing AI models can be improved by considering comorbidity as an independent factor. Furthermore, ARDS post-processing clinical systems must involve include (i) the clinical validation and verification of AI-models, (ii) reliability and stability criteria, and (iii) easily adaptable, and (iv) generalization assessments of AI systems for their use in pulmonary, critical care, and radiological settings.
截至 2020 年 12 月 21 日,COVID-19 已在全球范围内感染了 7740 万人,并导致 170 万人死亡。COVID-19 导致死亡的主要原因是急性呼吸窘迫综合征(ARDS)。根据世界卫生组织(WHO)的说法,至少 60 岁或患有主要针对的合并症的人感染 SARS-CoV-2 的风险最高。在当前持续的大流行期间,医学成像提供了一种非侵入性、无接触且相对更安全的诊断替代工具。人工智能(AI)科学家正在开发多种智能计算机辅助诊断(CAD)工具,应用于多种成像模式,即肺部计算机断层扫描(CT)、胸部 X 射线和肺部超声。这些 AI 工具通过以下方式帮助肺部和重症监护临床医生:(a)更快地检测病毒的存在,(b)对肺炎类型进行分类,以及(c)测量 COVID-19 感染患者的病毒损伤严重程度。因此,充分了解快速、成功和及时进行肺部扫描分析的要求至关重要。本叙述性评论首先介绍了 COVID-19 情况下肺部的病理布局,然后理解并解释了 ARDS 框架中的合并症统计分布。本综述的新颖之处在于根据思想流派(SoT)对 AI 模型进行分类的方法,根据技术及其特征的隔离进行展示。该研究还讨论了基于非 ARDS 肺部(COVID-19 之前)到 ARDS 肺部(COVID-19 之后)对 AI 模型的识别及其扩展。此外,它还介绍了 COVID-19 框架中医疗成像模式的 AI 工作流程考虑因素。最后,将讨论临床 AI 设计注意事项。我们的结论是,通过将合并症视为独立因素,可以改进当前 AI 模型的设计。此外,ARDS 后处理临床系统必须包括:(i)对 AI 模型进行临床验证和验证,(ii)可靠性和稳定性标准,以及(iii)易于适应和(iv)用于肺部、重症监护和放射学环境的 AI 系统的泛化评估。