Goldsmith Ira, Chesterfield-Thomas Gemma, Toghill Hannah
Department of Cardiothoracic Surgery, Morriston Hospital, Swansea, Wales SA6 6NL, UK.
Department of Physiotherapy, Morriston Hospital, Swansea, Wales SA6 6NL, UK.
EClinicalMedicine. 2020 Nov 30;31:100663. doi: 10.1016/j.eclinm.2020.100663. eCollection 2021 Jan.
Anatomical lung resection offers the best prospect of long-term survival in patients with non-small cell lung cancer (NSCLC). However, some patients with significant dyspnoea, impaired performance status (PS), borderline or poor pulmonary function are considered inoperable and instead referred for radiotherapy, chemotherapy or palliative care. The aims of the study were to determine whether pre-operative pulmonary physiotherapy (Prehab), by improving clinical parameters, (i) makes patients suitable for surgery who were considered inoperable on subjective criteria of dyspnoea >3 and PS >2, and objective criteria of diffusing capacity for carbon monoxide (DLCO) <50%; and (ii) thereby allows them to safely receive curative surgery with reduced morbidity and mortality.
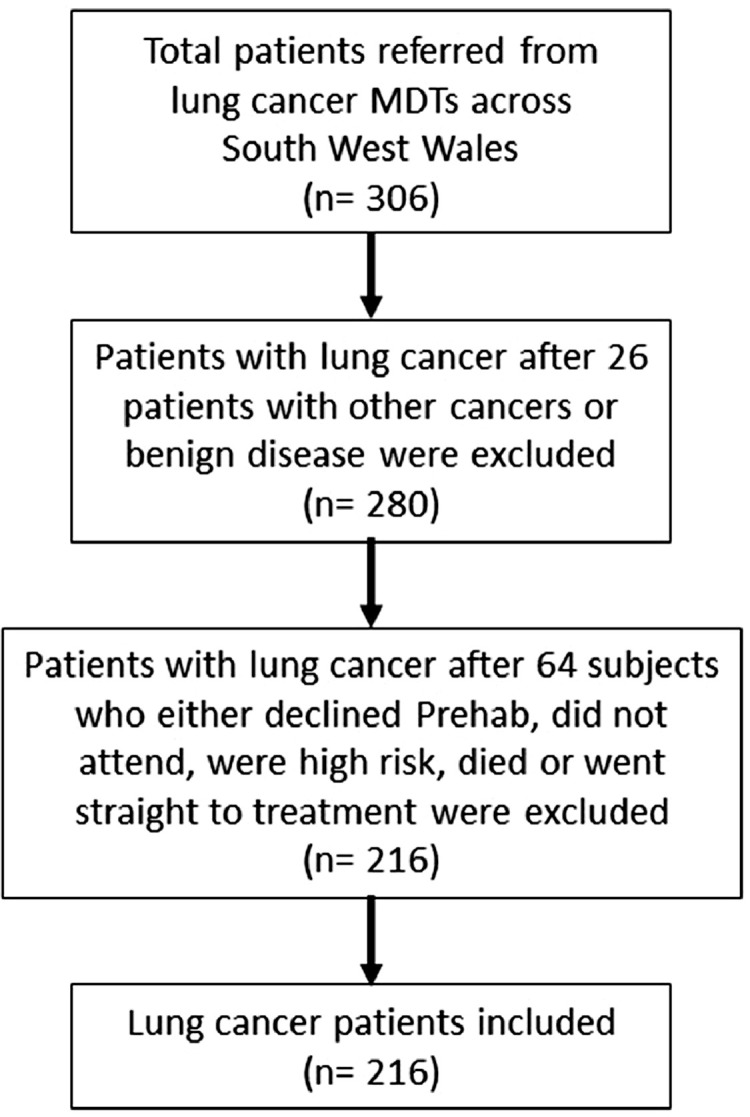
From January 2017 to December 2018 a total of 306 patients were prospectively and sequentially assessed for Prehab and 216 patients with lung cancer studied. Their mean age (95% CI) was 71.7 ± 1.1 years, 50.5% ( = 109) were men and they received Prehab over 39.0 ± 7.0 days averaging 3.1 ± 0.6 sessions. Their dyspnoea scores, PS, level of activity, six minute walk test (6MWT) and frailty index prior to and following Prehab were determined. Following surgery the post-operative length of hospital stay (LOHS), complications and mortality at 30 days, 90 days and 1 year determined. Similar outcomes were determined for (i) high-risk patients with dyspnoea scores >3 and PS >2, and compared with low-risk patients having dyspnoea scores <2 and PS <2 (subjective criteria); and (ii) high-risk patients with DLCO <50% and compared with low-risk patients with DLCO >80% (objective criteria).
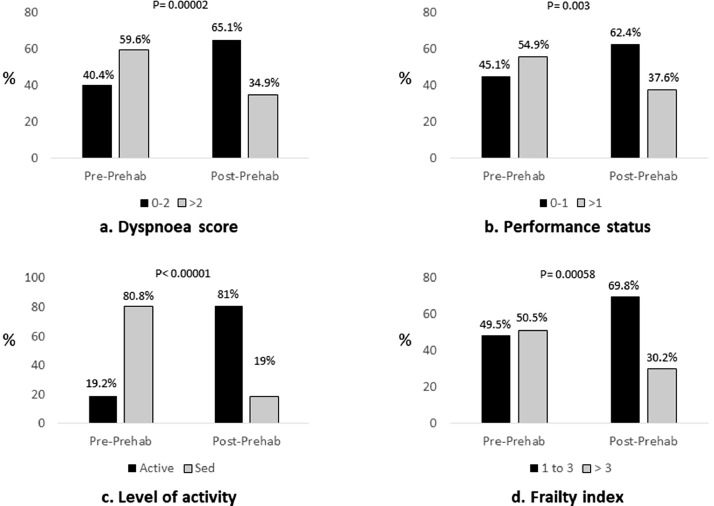
In the total cohort following Prehab, there was significant improvement in the dyspnoea scores <2 / ≥2 (40%/60% prior to Prehab vs. 65%/35% following Prehab, = 0.00002), PS <2 / ≥2 (45%/55% prior to vs. 62%/38% following Prehab, = 0.003), frailty index ≤3 / >3 (49%/51% vs 70%/30%, = 0.0006), and 6MWT (306.6 ± 6.8 m vs 354.8 ± 52.7 m, = 0.04). Post-operative major complication rates were 8.7%; median LOHS was 7 (IQR 6) days; hospital mortality at 30 days 1.3%, 90 days 4.7% and 1 year 16%. Using subjective criteria of dyspnoea scores >3 and PS >2, 100% of high-risk patients were considered inoperable. Following optimization with Prehab 84.2% of the high-risk patients were ready to proceed with radical treatment and 52.6% with surgery, and subsequently 42.8% of patients underwent surgery. Likewise, 78.8% of patients with DLCO <50% were considered inoperable. Following Prehab 86.5% of high-risk patients were ready to proceed with radical treatment and 59.1% with surgery, and 54.6% of high-risk patients underwent surgery. In each category there were no significant differences in complications, LOHS or mortality rates between the high-risk and low-risk patients.
Our prospective study showed that with Prehab there was clinical and statistically significant improvement in the dyspnoea scores, PS, level of activity and frailty, particularly in the high-risk group of patients. Importantly, Prehab made previously inoperable patients operable, allowing them to safely undergo curative lung resection. This strategy helps improve resection rates and may contribute to the long term survival of lung cancer patients.
This is a Welsh Health Specialised Services Committee (WHSSC) commissioned service.
解剖性肺切除术为非小细胞肺癌(NSCLC)患者提供了最佳的长期生存前景。然而,一些有明显呼吸困难、功能状态(PS)受损、肺功能临界或较差的患者被认为无法进行手术,转而接受放疗、化疗或姑息治疗。本研究的目的是确定术前肺康复治疗(Prehab)是否通过改善临床参数,(i)使那些根据主观标准呼吸困难评分>3且PS>2,以及客观标准一氧化碳弥散量(DLCO)<50%而被认为无法手术的患者适合手术;(ii)从而使他们能够安全地接受根治性手术,同时降低发病率和死亡率。
从2017年1月至2018年12月,对总共306例患者进行了前瞻性和序贯性的Prehab评估,其中216例肺癌患者纳入研究。他们的平均年龄(95%CI)为71.7±1.1岁,50.5%(n = 109)为男性,他们接受Prehab治疗的时间为39.0±7.0天,平均治疗3.1±0.6个疗程。测定了他们在Prehab治疗前后的呼吸困难评分、PS、活动水平、六分钟步行试验(6MWT)和衰弱指数。手术后,确定术后住院时间(LOHS)、30天、90天和1年时的并发症及死亡率。对(i)呼吸困难评分>3且PS>2的高危患者进行了类似结果的测定,并与呼吸困难评分<2且PS<2的低危患者(主观标准)进行比较;(ii)DLCO<50%的高危患者进行了类似结果的测定,并与DLCO>80%的低危患者(客观标准)进行比较。
在整个队列中,经过Prehab治疗后,呼吸困难评分<2/≥2(Prehab治疗前为40%/60%,治疗后为65%/35%,P = 0.00002)、PS<2/≥2(治疗前为45%/55%,治疗后为62%/38%,P = 0.003)、衰弱指数≤3/>3(49%/51%对70%/30%,P = 0.0006)以及6MWT(306.6±6.8米对354.8±52.7米,P = 0.04)均有显著改善。术后主要并发症发生率为8.7%;中位LOHS为7(IQR 6)天;30天医院死亡率为1.3%,90天为4.7%,1年为16%。采用呼吸困难评分>3且PS>2的主观标准,100%的高危患者被认为无法手术。经过Prehab优化后,84.2%的高危患者准备进行根治性治疗,52.6%准备进行手术,随后42.8%的患者接受了手术。同样,78.8%的DLCO<50%的患者被认为无法手术。经过Prehab治疗后,86.5%的高危患者准备进行根治性治疗,59.1%准备进行手术,54.6%的高危患者接受了手术。在每个类别中,高危患者和低危患者在并发症、LOHS或死亡率方面均无显著差异。
我们的前瞻性研究表明,通过Prehab治疗,呼吸困难评分、PS、活动水平和衰弱程度在临床和统计学上均有显著改善,特别是在高危患者组中。重要的是,Prehab使先前无法手术的患者能够接受手术,从而使他们能够安全地进行根治性肺切除术。这一策略有助于提高切除率,并可能有助于肺癌患者的长期生存。
这是威尔士卫生专业服务委员会(WHSSC)委托开展的一项服务。