Harvard John A. Paulson School of Engineering and Applied Science, Harvard University, Cambridge, MA, USA.
Department of Environmental Health, Harvard T.H. Chan School of Public Heath, Boston, MA, USA.
Respir Res. 2021 Feb 26;22(1):73. doi: 10.1186/s12931-021-01637-8.
The mechanism for spread of SARS-CoV-2 has been attributed to large particles produced by coughing and sneezing. There is controversy whether smaller airborne particles may transport SARS-CoV-2. Smaller particles, particularly fine particulate matter (≤ 2.5 µm in diameter), can remain airborne for longer periods than larger particles and after inhalation will penetrate deeply into the lungs. Little is known about the size distribution and location of airborne SARS-CoV-2 RNA.
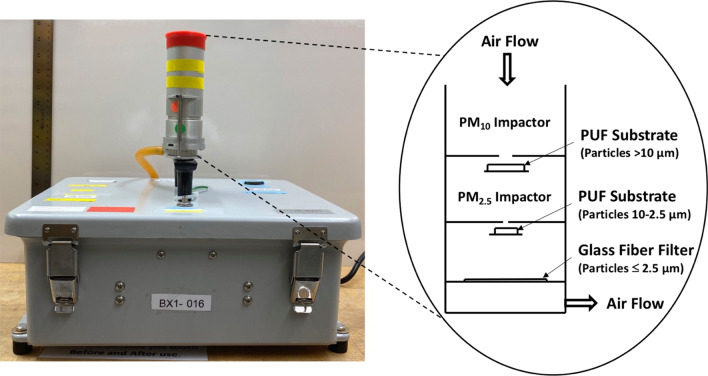
As a measure of hospital-related exposure, air samples of three particle sizes (> 10.0 µm, 10.0-2.5 µm, and ≤ 2.5 µm) were collected in a Boston, Massachusetts (USA) hospital from April to May 2020 (N = 90 size-fractionated samples). Locations included outside negative-pressure COVID-19 wards, a hospital ward not directly involved in COVID-19 patient care, and the emergency department.
SARS-CoV-2 RNA was present in 9% of samples and in all size fractions at concentrations of 5 to 51 copies m. Locations outside COVID-19 wards had the fewest positive samples. A non-COVID-19 ward had the highest number of positive samples, likely reflecting staff congregation. The probability of a positive sample was positively associated (r = 0.95, p < 0.01) with the number of COVID-19 patients in the hospital. The number of COVID-19 patients in the hospital was positively associated (r = 0.99, p < 0.01) with the number of new daily cases in Massachusetts.
More frequent detection of positive samples in non-COVID-19 than COVID-19 hospital areas indicates effectiveness of COVID-ward hospital controls in controlling air concentrations and suggests the potential for disease spread in areas without the strictest precautions. The positive associations regarding the probability of a positive sample, COVID-19 cases in the hospital, and cases in Massachusetts suggests that hospital air sample positivity was related to community burden. SARS-CoV-2 RNA with fine particulate matter supports the possibility of airborne transmission over distances greater than six feet. The findings support guidelines that limit exposure to airborne particles including fine particles capable of longer distance transport and greater lung penetration.
SARS-CoV-2 的传播机制归因于咳嗽和打喷嚏产生的大颗粒。较小的空气传播颗粒是否可能传播 SARS-CoV-2 存在争议。较小的颗粒,特别是细颗粒物(直径≤2.5μm),比大颗粒在空中停留的时间更长,并且在吸入后会深入肺部。关于空气传播 SARS-CoV-2 RNA 的粒径分布和位置知之甚少。
作为医院相关暴露的衡量标准,2020 年 4 月至 5 月,在美国马萨诸塞州波士顿的一家医院采集了三种粒径(>10.0μm、10.0-2.5μm 和≤2.5μm)的空气样本(N=90 个粒径分级样本)。采样地点包括负压 COVID-19 病房外、不直接参与 COVID-19 患者护理的医院病房和急诊部。
SARS-CoV-2 RNA 存在于 9%的样本中,浓度为 5 到 51 拷贝/m 的所有粒径分数中。COVID-19 病房外的采样地点阳性样本最少。非 COVID-19 病房的阳性样本数量最多,可能反映了工作人员的聚集。阳性样本的概率与医院内 COVID-19 患者的数量呈正相关(r=0.95,p<0.01)。医院内 COVID-19 患者的数量与马萨诸塞州每日新增病例数呈正相关(r=0.99,p<0.01)。
在非 COVID-19 医院区域比 COVID-19 医院区域更频繁地检测到阳性样本,表明 COVID-19 病房医院控制措施有效,控制空气浓度,并表明在没有最严格预防措施的区域有疾病传播的潜力。关于阳性样本概率、医院内 COVID-19 病例数和马萨诸塞州病例数的正相关关系表明,医院空气样本的阳性与社区负担有关。与细颗粒物一起的 SARS-CoV-2 RNA 支持超过六英尺距离的空气传播的可能性。这些发现支持了限制包括能够远距离传输和更深入肺部的细颗粒在内的空气传播颗粒暴露的指南。