Stremmel Christopher, Scherer Clemens, Lüsebrink Enzo, Kupka Danny, Schmid Teresa, Stocker Thomas, Kellnar Antonia, Kleeberger Jan, Sinner Moritz F, Petzold Tobias, Mehilli Julinda, Braun Daniel, Orban Mathias, Hausleiter Jörg, Massberg Steffen, Orban Martin
Medizinische Klinik und Poliklinik I, Klinikum der Universität München, Munich, Germany.
DZHK (German Centre for Cardiovascular Research), partner site Munich Heart Alliance, Klinikum der Universität München, Munich, Germany.
Int J Cardiol Heart Vasc. 2021 Feb 5;32:100722. doi: 10.1016/j.ijcha.2021.100722. eCollection 2021 Feb.
Acute cardiac tamponade is a life-threatening pathology in modern cardiology as catheter-based interventions become increasingly relevant. Pericardiocentesis is usually the primary treatment of choice. However, protocols for handling of draining pigtail catheters are very variable due to limit data and require further investigation.
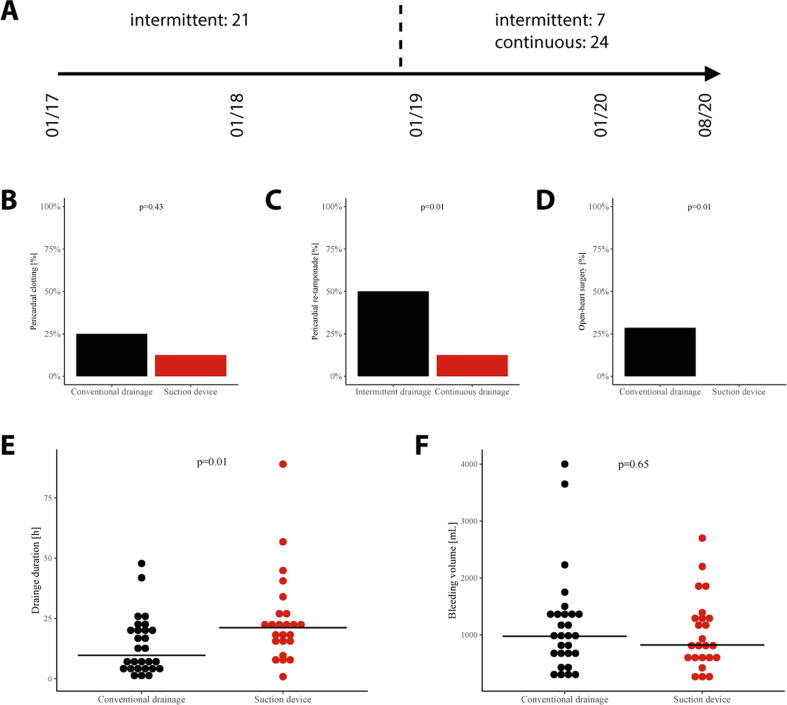
We retrospectively analyzed 52 patients with acute cardiac tamponade requiring immediate pericardiocentesis from January 2017 to August 2020. Patients were treated with a classical approach of intermittent manual aspiration or continuous pericardial drainage using a redon drainage system.
Mean age of patients was 74 years in both groups. Most common causes for cardiac tamponade were percutaneous coronary interventions in about 50% and transaortic valve implantations in 25% of all cases. 28 patients were treated with classic intermittent drainage from 2017 to 2020. 24 patients were treated with continuous drainage from December 2018-2020. Compared to classical intermittent drainage treatment, continuous drainage was associated with a lower rate of a surgical intervention or cardiac re-tamponade and a lower mortality at 5 days (HR 0.2, 95% CI 0.1-0.9, log-rank p = 0.03). Despite a longer total drainage time under continuous suction, drainage volumes were comparable in both groups.
Acute cardiac tamponade can be efficiently treated by pericardiocentesis with subsequent continuous negative pressure drainage via a pigtail catheter. Our retrospective analysis shows a significantly lower mortality, a decreased rate of interventions and lower rates of cardiac re-tamponade without any relevant side effects when compared to classical intermittent manual drainage. These findings require further investigations in larger, randomized trials.
在现代心脏病学中,随着基于导管的介入治疗越来越普遍,急性心脏压塞是一种危及生命的病症。心包穿刺术通常是首选的主要治疗方法。然而,由于数据有限,处理引流猪尾导管的方案差异很大,需要进一步研究。
我们回顾性分析了2017年1月至2020年8月期间52例需要立即进行心包穿刺术的急性心脏压塞患者。患者采用间歇性手动抽吸的经典方法或使用雷顿引流系统进行持续心包引流治疗。
两组患者的平均年龄均为74岁。心脏压塞最常见的原因是经皮冠状动脉介入治疗,约占所有病例的50%,经主动脉瓣植入术占25%。2017年至2020年,28例患者接受了经典的间歇性引流治疗。2018年12月至2020年,24例患者接受了持续引流治疗。与经典的间歇性引流治疗相比,持续引流与手术干预或心脏再压塞的发生率较低以及5天时的死亡率较低相关(风险比0.2,95%置信区间0.1 - 0.9,对数秩检验p = 0.03)。尽管持续抽吸下的总引流时间较长,但两组的引流量相当。
急性心脏压塞可通过心包穿刺术有效治疗,随后通过猪尾导管进行持续负压引流。我们的回顾性分析表明,与经典的间歇性手动引流相比,死亡率显著降低,干预率降低,心脏再压塞率降低,且无任何相关副作用。这些发现需要在更大规模的随机试验中进一步研究。