School of Medicine, Emory University, Atlanta, Georgia.
Rollins School of Public Health, Emory University, Atlanta, Georgia.
JAMA Netw Open. 2021 Mar 1;4(3):e211283. doi: 10.1001/jamanetworkopen.2021.1283.
Risks for severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection among health care personnel (HCP) are unclear.
To evaluate the risk factors associated with SARS-CoV-2 seropositivity among HCP with the a priori hypothesis that community exposure but not health care exposure was associated with seropositivity.
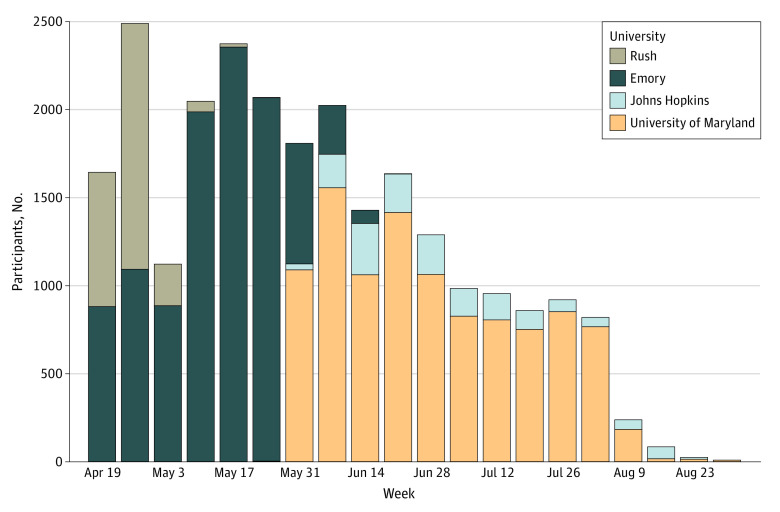
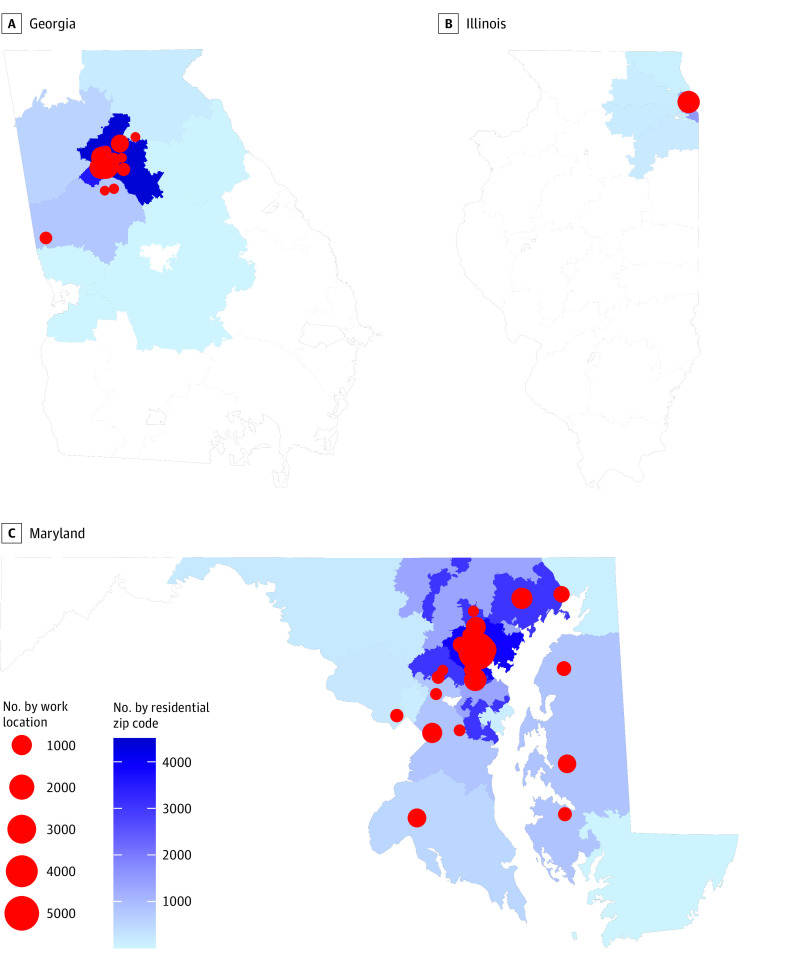
DESIGN, SETTING, AND PARTICIPANTS: This cross-sectional study was conducted among volunteer HCP at 4 large health care systems in 3 US states. Sites shared deidentified data sets, including previously collected serology results, questionnaire results on community and workplace exposures at the time of serology, and 3-digit residential zip code prefix of HCP. Site-specific responses were mapped to a common metadata set. Residential weekly coronavirus disease 2019 (COVID-19) cumulative incidence was calculated from state-based COVID-19 case and census data.
Model variables included demographic (age, race, sex, ethnicity), community (known COVID-19 contact, COVID-19 cumulative incidence by 3-digit zip code prefix), and health care (workplace, job role, COVID-19 patient contact) factors.
The main outcome was SARS-CoV-2 seropositivity. Risk factors for seropositivity were estimated using a mixed-effects logistic regression model with a random intercept to account for clustering by site.
Among 24 749 HCP, most were younger than 50 years (17 233 [69.6%]), were women (19 361 [78.2%]), were White individuals (15 157 [61.2%]), and reported workplace contact with patients with COVID-19 (12 413 [50.2%]). Many HCP worked in the inpatient setting (8893 [35.9%]) and were nurses (7830 [31.6%]). Cumulative incidence of COVID-19 per 10 000 in the community up to 1 week prior to serology testing ranged from 8.2 to 275.6; 20 072 HCP (81.1%) reported no COVID-19 contact in the community. Seropositivity was 4.4% (95% CI, 4.1%-4.6%; 1080 HCP) overall. In multivariable analysis, community COVID-19 contact and community COVID-19 cumulative incidence were associated with seropositivity (community contact: adjusted odds ratio [aOR], 3.5; 95% CI, 2.9-4.1; community cumulative incidence: aOR, 1.8; 95% CI, 1.3-2.6). No assessed workplace factors were associated with seropositivity, including nurse job role (aOR, 1.1; 95% CI, 0.9-1.3), working in the emergency department (aOR, 1.0; 95% CI, 0.8-1.3), or workplace contact with patients with COVID-19 (aOR, 1.1; 95% CI, 0.9-1.3).
In this cross-sectional study of US HCP in 3 states, community exposures were associated with seropositivity to SARS-CoV-2, but workplace factors, including workplace role, environment, or contact with patients with known COVID-19, were not. These findings provide reassurance that current infection prevention practices in diverse health care settings are effective in preventing transmission of SARS-CoV-2 from patients to HCP.
医护人员(HCP)感染严重急性呼吸系统综合症冠状病毒 2(SARS-CoV-2)的风险尚不清楚。
评估与 HCP 中 SARS-CoV-2 血清阳性相关的风险因素,假设社区暴露而非医疗保健暴露与血清阳性相关。
设计、地点和参与者:本横断面研究在 3 个美国州的 4 个大型医疗保健系统中的志愿 HCP 中进行。各站点共享经身份识别的数据组,包括先前收集的血清学结果、血清学检测时社区和工作场所暴露的问卷调查结果以及 HCP 的 3 位邮政编码前缀。站点特异性响应映射到公共元数据集。从基于州的 COVID-19 病例和人口普查数据计算每周 COVID-19 的累积发病率。
模型变量包括人口统计学(年龄、种族、性别、族裔)、社区(已知的 COVID-19 接触、按 3 位邮政编码前缀的 COVID-19 累积发病率)和医疗保健(工作场所、工作角色、COVID-19 患者接触)因素。
主要结果是 SARS-CoV-2 血清阳性。使用混合效应逻辑回归模型估计血清阳性的风险因素,该模型具有随机截距,以考虑站点聚类。
在 24749 名 HCP 中,大多数年龄小于 50 岁(17233 [69.6%]),为女性(19361 [78.2%]),为白人个体(15157 [61.2%]),并报告在工作场所接触过 COVID-19 患者(12413 [50.2%])。许多 HCP 在住院环境中工作(8893 [35.9%]),是护士(7830 [31.6%])。在血清学检测前 1 周内,社区中每 10000 人 COVID-19 的累积发病率范围为 8.2 至 275.6;20072 名 HCP(81.1%)报告在社区中没有 COVID-19 接触。总体血清阳性率为 4.4%(95%CI,4.1%-4.6%;1080 名 HCP)。在多变量分析中,社区 COVID-19 接触和社区 COVID-19 累积发病率与血清阳性相关(社区接触:调整后的优势比 [aOR],3.5;95%CI,2.9-4.1;社区累积发病率:aOR,1.8;95%CI,1.3-2.6)。评估的工作场所因素均与血清阳性无关,包括护士工作角色(aOR,1.1;95%CI,0.9-1.3)、在急诊室工作(aOR,1.0;95%CI,0.8-1.3)或与已知 COVID-19 患者在工作场所接触(aOR,1.1;95%CI,0.9-1.3)。
在这项对美国 3 个州的 HCP 的横断面研究中,社区暴露与 SARS-CoV-2 血清阳性相关,但工作场所因素(包括工作场所角色、环境或与已知 COVID-19 患者接触)则不然。这些发现表明,目前在不同医疗保健环境中实施的感染预防措施可有效防止 SARS-CoV-2 从患者传播给 HCP。