Gilbert Ileen, Aslam Mahmood Aanam, Devane Katie, Tan Laren
AstraZeneca, Wilmington, DE, USA.
IQVIA, Durham, NC, USA.
Pulm Ther. 2021 Jun;7(1):189-201. doi: 10.1007/s41030-021-00147-8. Epub 2021 Mar 12.
There are limited data on the effects of forced medication switching for a nonmedical reason in patients with obstructive airway conditions. This study evaluated disruption in care resulting from a nonmedical medication switch for patients with asthma and/or chronic obstructive pulmonary disease who previously received the inhaled corticosteroid/long-acting β-agonist budesonide/formoterol.
This retrospective pharmacy benefit prescription claims analysis evaluated Medicare Part D patients who filled a prescription for budesonide/formoterol as their last inhaled corticosteroid/long-acting β-agonist in 2016 and were affected by a formulary block of budesonide/formoterol in 2017. Changes to respiratory maintenance therapy, length of gaps in care during which a patient was not in possession of a respiratory controller medication, acute medication use indicative of disease exacerbations, and medication adherence were assessed.
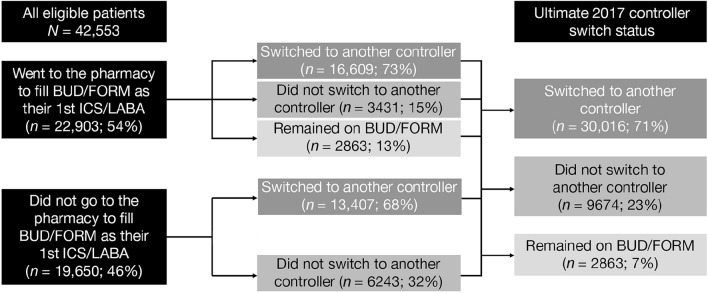
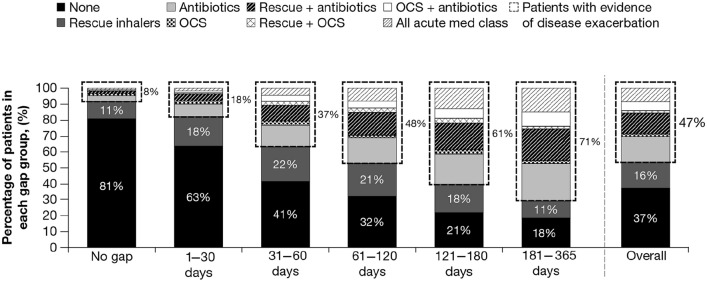
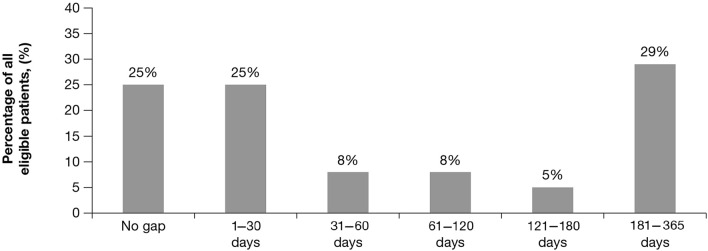
A total of 42,553 patients were included in the analysis. Following the formulary block, 30,016 patients (71%) switched to another controller; 20,628 of these patients (69%) switched to a new inhaled corticosteroid/long-acting β-agonist, 7081 (23%) stepped down to a monotherapy, and 2307 (8%) switched to a non-inhaled corticosteroid-containing controller. Despite the formulary block, 22,903 patients (54%) attempted to fill budesonide/formoterol as their first postblock controller, and 6624 patients (16%) attempted to return to budesonide/formoterol after switching to another controller. On average, patients experienced a gap in care of approximately 4 months without a controller medication. Also, 9674 (23%) did not fill any controller over the 1-year postblock period. Of those patients who experienced a gap in care, 14,926 (47%) filled a prescription indicative of a possible exacerbation during the gap period (i.e., oral corticosteroids for patients with asthma and oral corticosteroids and/or antibiotics for patients with chronic obstructive pulmonary disease).
The Medicare Part D formulary block was associated with disruption in the management of patients' respiratory conditions and may have adversely impacted disease control.
关于因非医疗原因强制更换药物对气道阻塞性疾病患者的影响,相关数据有限。本研究评估了非医疗原因导致的药物更换对哮喘和/或慢性阻塞性肺疾病患者护理的干扰,这些患者之前使用吸入性糖皮质激素/长效β受体激动剂布地奈德/福莫特罗。
这项回顾性药房福利处方索赔分析评估了2016年最后一次将布地奈德/福莫特罗作为吸入性糖皮质激素/长效β受体激动剂开具处方且在2017年受到布地奈德/福莫特罗药品目录限制影响的医疗保险D部分患者。评估了呼吸维持治疗的变化、患者未持有呼吸控制药物期间的护理中断时长、疾病加重的急性药物使用情况以及药物依从性。
共有42553名患者纳入分析。在药品目录限制之后,30016名患者(71%)更换为另一种控制药物;其中20628名患者(69%)更换为新的吸入性糖皮质激素/长效β受体激动剂,7081名(23%)降级为单一疗法,2307名(8%)更换为不含吸入性糖皮质激素的控制药物。尽管有药品目录限制,22903名患者(54%)试图将布地奈德/福莫特罗作为限制后的第一种控制药物开具处方,6624名患者(16%)在更换为另一种控制药物后试图重新使用布地奈德/福莫特罗。平均而言,患者在没有控制药物的情况下经历了约4个月的护理中断。此外,9674名(23%)患者在限制后1年期间未开具任何控制药物处方。在经历护理中断的患者中,14926名(47%)在中断期间开具了可能提示病情加重的处方(即哮喘患者使用口服糖皮质激素,慢性阻塞性肺疾病患者使用口服糖皮质激素和/或抗生素)。
医疗保险D部分药品目录限制与患者呼吸疾病管理的中断相关,可能对疾病控制产生不利影响。