Salter Amber, Fox Robert J, Newsome Scott D, Halper June, Li David K B, Kanellis Pamela, Costello Kathleen, Bebo Bruce, Rammohan Kottil, Cutter Gary R, Cross Anne H
Washington University School of Medicine in St Louis, St Louis, Missouri.
Cleveland Clinic, Cleveland, Ohio.
JAMA Neurol. 2021 Jun 1;78(6):699-708. doi: 10.1001/jamaneurol.2021.0688.
Emergence of SARS-CoV-2 causing COVID-19 prompted the need to gather information on clinical outcomes and risk factors associated with morbidity and mortality in patients with multiple sclerosis (MS) and concomitant SARS-CoV-2 infections.
To examine outcomes and risk factors associated with COVID-19 clinical severity in a large, diverse cohort of North American patients with MS.
DESIGN, SETTING, AND PARTICIPANTS: This analysis used deidentified, cross-sectional data on patients with MS and SARS-CoV-2 infection reported by health care professionals in North American academic and community practices between April 1, 2020, and December 12, 2020, in the COVID-19 Infections in MS Registry. Health care professionals were asked to report patients after a minimum of 7 days from initial symptom onset and after sufficient time had passed to observe the COVID-19 disease course through resolution of acute illness or death. Data collection began April 1, 2020, and is ongoing.
Laboratory-positive SARS-CoV-2 infection or highly suspected COVID-19.
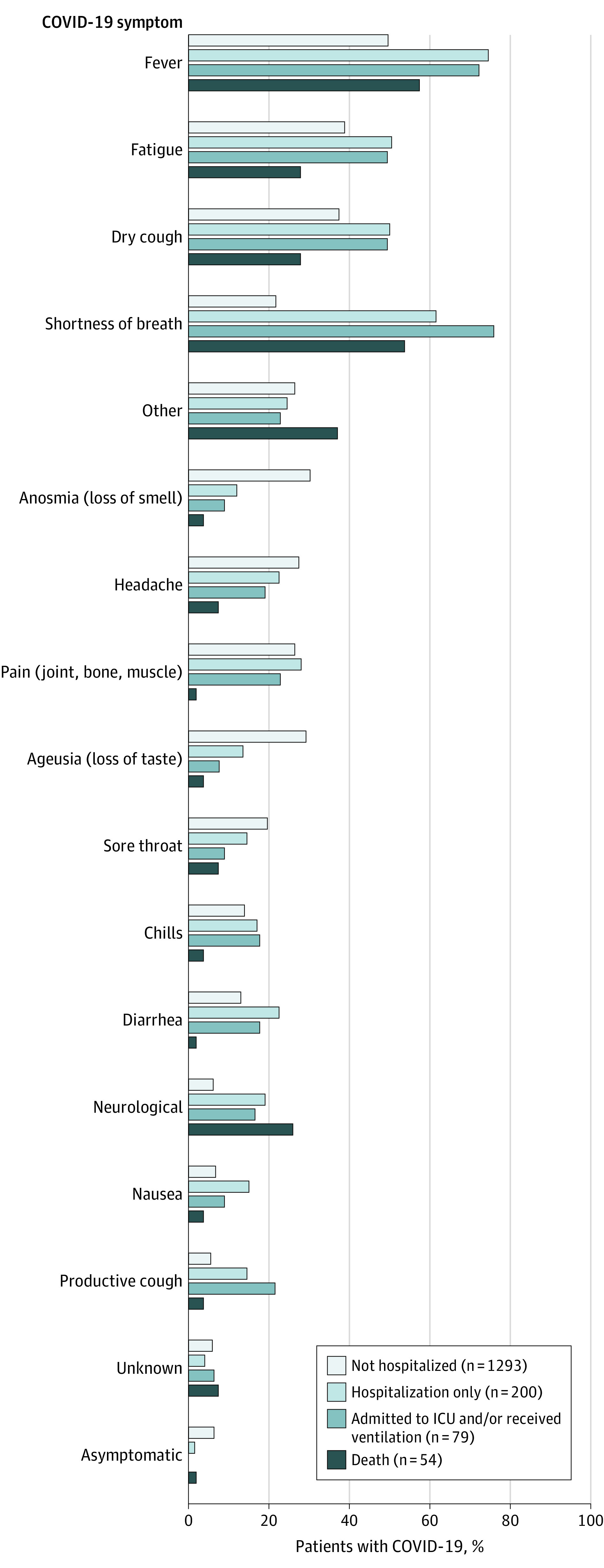
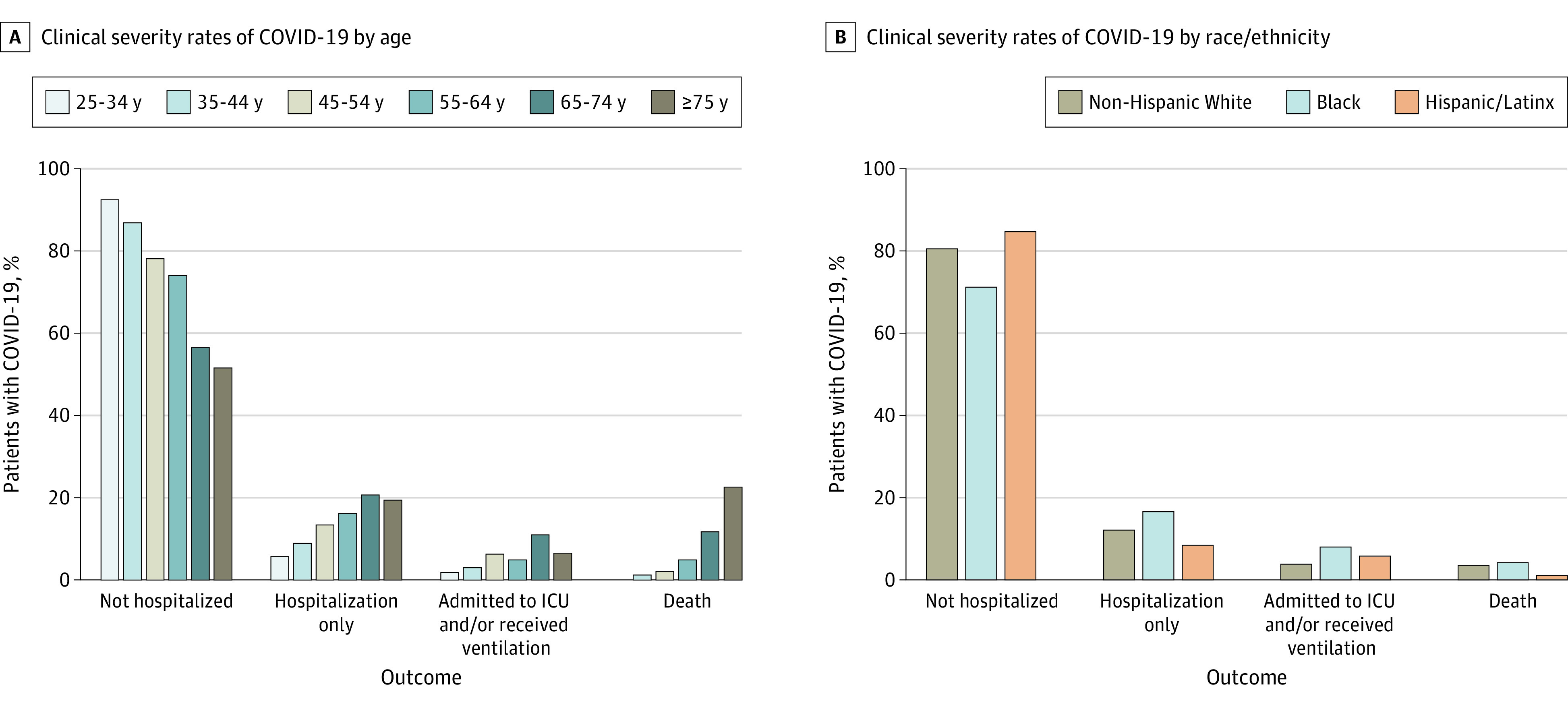
Clinical outcome with 4 levels of increasing severity: not hospitalized, hospitalization only, admission to the intensive care unit and/or required ventilator support, and death.
Of 1626 patients, most had laboratory-positive SARS-CoV-2 infection (1345 [82.7%]), were female (1202 [74.0%]), and had relapsing-remitting MS (1255 [80.4%]). A total of 996 patients (61.5%) were non-Hispanic White, 337 (20.8%) were Black, and 190 (11.7%) were Hispanic/Latinx. The mean (SD) age was 47.7 (13.2) years, and 797 (49.5%) had 1 or more comorbidity. The overall mortality rate was 3.3% (95% CI, 2.5%-4.3%). Ambulatory disability and older age were each independently associated with increased odds of all clinical severity levels compared with those not hospitalized after adjusting for other risk factors (nonambulatory: hospitalization only, odds ratio [OR], 2.8 [95% CI, 1.6-4.8]; intensive care unit/required ventilator support, OR, 3.5 [95% CI, 1.6-7.8]; death, OR, 25.4 [95% CI, 9.3-69.1]; age [every 10 years]: hospitalization only, OR, 1.3 [95% CI, 1.1-1.6]; intensive care unit/required ventilator support, OR, 1.3 [95% CI, 0.99-1.7]; death, OR, 1.8 [95% CI, 1.2-2.6]).
In this registry-based cross-sectional study, increased disability was independently associated with worse clinical severity including death from COVID-19. Other risk factors for worse outcomes included older age, Black race, cardiovascular comorbidities, and recent treatment with corticosteroids. Knowledge of these risk factors may improve the treatment of patients with MS and COVID-19 by helping clinicians identify patients requiring more intense monitoring or COVID-19 treatment.
严重急性呼吸综合征冠状病毒2(SARS-CoV-2)引发2019冠状病毒病(COVID-19),促使人们需要收集有关多发性硬化症(MS)患者合并SARS-CoV-2感染的临床结局以及与发病和死亡相关的风险因素的信息。
在北美一大群多样化的MS患者中,研究与COVID-19临床严重程度相关的结局和风险因素。
设计、背景和参与者:本分析使用了去识别化的横断面数据,这些数据来自2020年4月1日至2020年12月12日期间北美学术和社区医疗机构的医护人员报告的MS和SARS-CoV-2感染患者,数据来自MS注册中心的COVID-19感染数据库。要求医护人员在患者出现初始症状至少7天后,以及经过足够时间观察COVID-19疾病进程直至急性疾病缓解或死亡后报告患者情况。数据收集于2020年4月1日开始,目前仍在进行。
实验室确诊的SARS-CoV-2感染或高度疑似的COVID-19。
临床结局分为4个严重程度递增的级别:未住院、仅住院、入住重症监护病房和/或需要呼吸机支持、死亡。
在1626例患者中,大多数患者实验室确诊为SARS-CoV-2感染(1345例[82.7%]),女性患者居多(1202例[74.0%]),且为复发缓解型MS(1255例[80.4%])。共有996例患者(61.5%)为非西班牙裔白人,337例(20.8%)为黑人,190例(11.7%)为西班牙裔/拉丁裔。平均(标准差)年龄为47.7(13.2)岁,797例(49.5%)有1种或更多合并症。总体死亡率为3.3%(95%置信区间,2.5%-4.3%)。在调整其他风险因素后,与未住院患者相比,行动不便和年龄较大各自独立与所有临床严重程度级别的几率增加相关(行动不便:仅住院,比值比[OR],2.8[95%置信区间,1.6-4.8];入住重症监护病房/需要呼吸机支持,OR,3.5[95%置信区间,1.6-7.8];死亡,OR,25.4[95%置信区间,9.3-69.1];年龄[每10岁]:仅住院,OR,1.3[95%置信区间,1.1-1.6];入住重症监护病房/需要呼吸机支持,OR,1.3[95%置信区间,0.99-1.7];死亡,OR,1.8[95%置信区间,1.2-2.6])。
在这项基于注册中心的横断面研究中,残疾程度增加与包括因COVID-19死亡在内的更差临床严重程度独立相关。其他不良结局的风险因素包括年龄较大、黑人种族、心血管合并症以及近期使用皮质类固醇治疗。了解这些风险因素可能有助于临床医生识别需要更密切监测或COVID-19治疗的患者,从而改善MS和COVID-19患者的治疗。