Department of Trauma and Orthopaedic Surgery, University Medical Center Hamburg-Eppendorf, Martinistrasse 52, 20246, Hamburg, Germany.
Department of Orthopaedic and Trauma Surgery, University Medical Center Schleswig-Holstein, Kiel, Germany.
Arch Orthop Trauma Surg. 2022 Mar;142(3):443-453. doi: 10.1007/s00402-021-03864-6. Epub 2021 Mar 22.
Although open-surgical techniques for the reconstruction of the posterolateral corner (PLC) are well established, the use of arthroscopic procedures has recently increased. When compared with open surgical preparation, arthroscopic orientation in the PLC is challenging and anatomic relations may not be familiar. Nevertheless, a profound knowledge of anatomic key structures and possible structures at risk as well as technical variations of arthroscopic approaches are mandatory to allow a precise and safe surgical intervention.
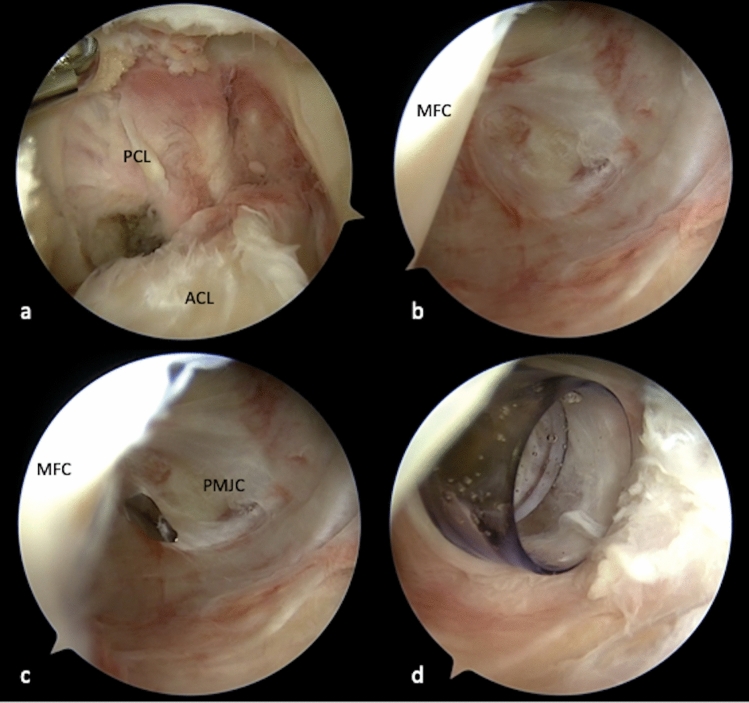
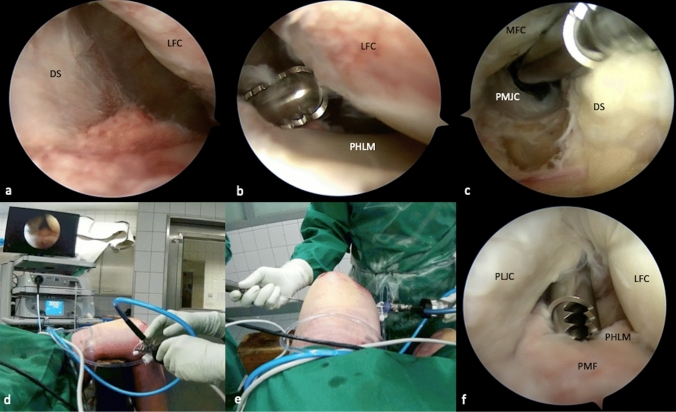
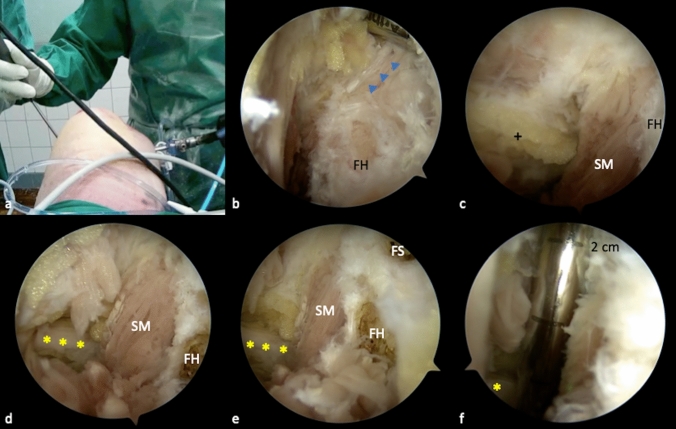
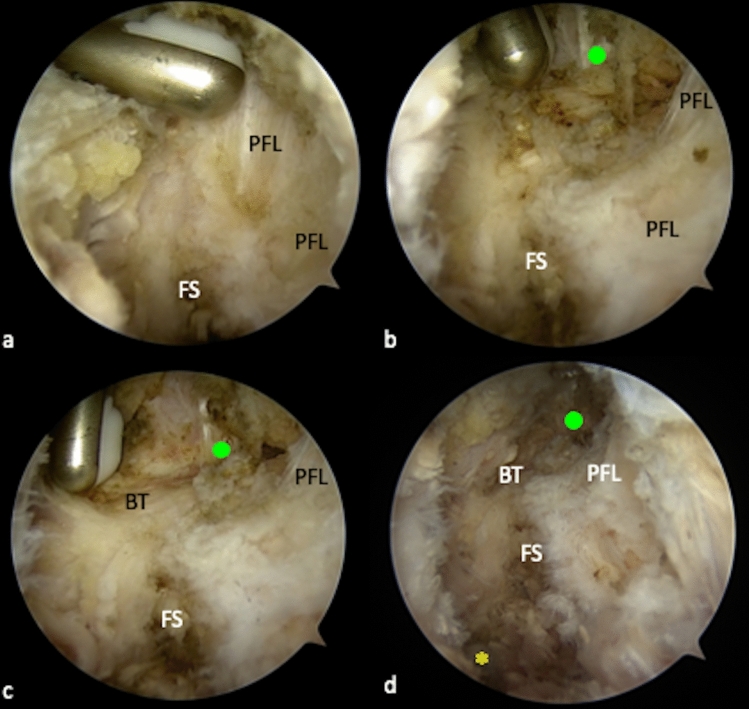
In a cadaveric video demonstration, an anterolateral (AL), anteromedial (AM), posteromedial (PM) and posterolateral (PL) portal, as well as a transseptal approach (TSA) were developed. Key structures of the PLC were defined and sequentially exposed during posterolateral arthroscopy. Finally, anatomic relations of all key structures were demonstrated.
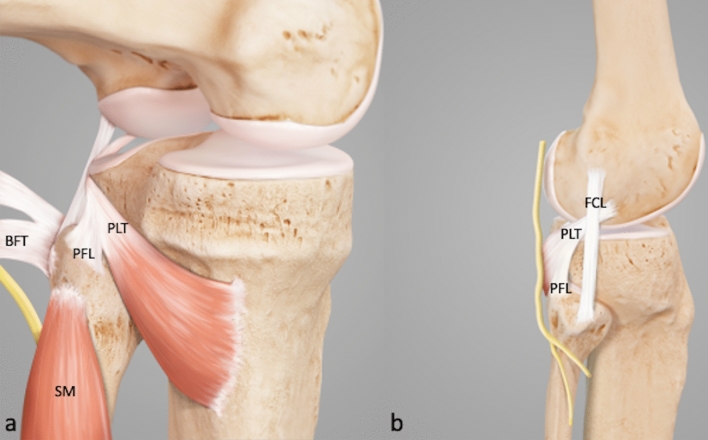
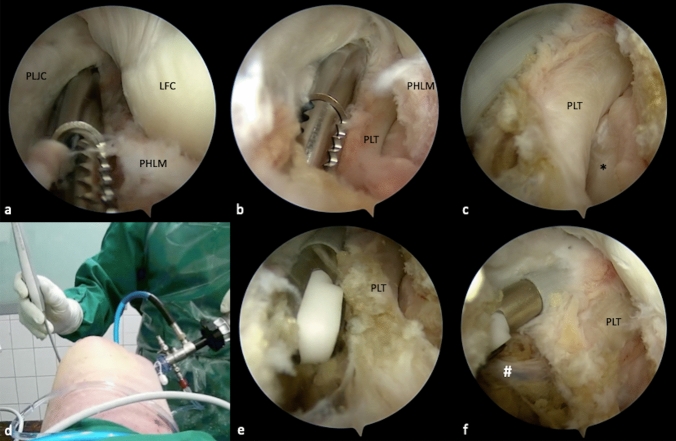
All key structures of the PLC can be visualized during arthroscopy. Thereby, careful portal placement is crucial in order to allow an effective exposure. Two alternatives of the TSA were described, depending on the region of interest. The peroneal nerve can be visualized dorsal to the biceps femoris tendon (BT), lateral to the soleus muscle (SM) and about 3 cm distal to the fibular styloid (FS). The distal attachment of the fibular collateral ligament (FCL) can be exposed on the lateral side of the fibular head (FH). The fibular attachment of the popliteofibular ligament (PFL) is exposed at the tip of the FS.
Arthroscopy of the posterolateral recessus allows full visualization of all key structures of the posterolateral corner, which provides the basis for anatomic and safe drill channel placement in PLC reconstruction. A sufficient exposure of relevant anatomic landmarks and precise portal preparation reduce the risk of iatrogenic vascular and peroneal nerve injury.
尽管开放手术技术已广泛应用于后外侧角(PLC)的重建,但关节镜技术的应用近来有所增加。与开放手术准备相比,PLC 关节镜定位具有挑战性,解剖关系可能不熟悉。然而,为了实现精确和安全的手术干预,必须深入了解解剖关键结构和可能的风险结构,以及关节镜入路的技术变化。
在尸体视频演示中,开发了前外侧(AL)、前内侧(AM)、后内侧(PM)和后外侧(PL)入路,以及经隔入路(TSA)。定义了 PLC 的关键结构,并在进行后外侧关节镜检查时依次暴露这些结构。最后,演示了所有关键结构的解剖关系。
所有 PLC 的关键结构均可在关节镜下可视化。因此,为了实现有效的暴露,仔细选择入路至关重要。根据感兴趣的区域,描述了 TSA 的两种替代方法。腓总神经可在比目鱼肌(SM)外侧、腓骨茎突(FS)远端 3 厘米处看到。外侧副韧带(LCL)的腓骨附着点可在腓骨头(FH)的外侧暴露。腘腓韧带(PFL)的腓骨附着点在 FS 的尖端暴露。
后外侧隐窝关节镜检查可全面观察 PLC 的所有关键结构,为 PLC 重建中安全的钻孔通道定位提供解剖学基础。充分暴露相关解剖标志和精确的入路准备可降低医源性血管和腓总神经损伤的风险。