Grill Katherine B, Wang Jichuan, Cheng Yao I, Lyon Maureen E
California Institute of Integral Studies, Department of Somatic Psychology, 1453 Mission Street, San Francisco, CA 94103.
Children's National Hospital, Children's National Research Institute, Center for Translational Research, 111 Michigan Ave. NW, Washington, DC 20010.
Psycholog Relig Spiritual. 2020 Nov;12(4):494-504. doi: 10.1037/rel0000301. Epub 2020 Jan 30.
Understanding how religion and spirituality influence health-related quality of life (HRQoL) is important for developing holistic, patient-centered treatment. This study determined distinct latent classes of religiousness/spirituality for adult persons living with HIV (PLWH) and associations between latent class membership and HRQoL.
Baseline data was collected from 223 patients in the FAmily CEntered (FACE) Advance Care Planning (ACP) clinical trial for PLWH. Patients completed the Brief Multidimensional Measurement of Religiousness/Spirituality (BMMRS-adapted), Patient Health Questionnaire (PHQ-9), Medical Outcome Study-HIV Survey (MOS-HIV) and the Palliative care Outcome Scale (POS). The optimal number of latent classes was determined by comparing K-Class model with (K-1)-Class model iteratively. The relationship between latent class membership, HRQoL and demographic characteristics was assessed.
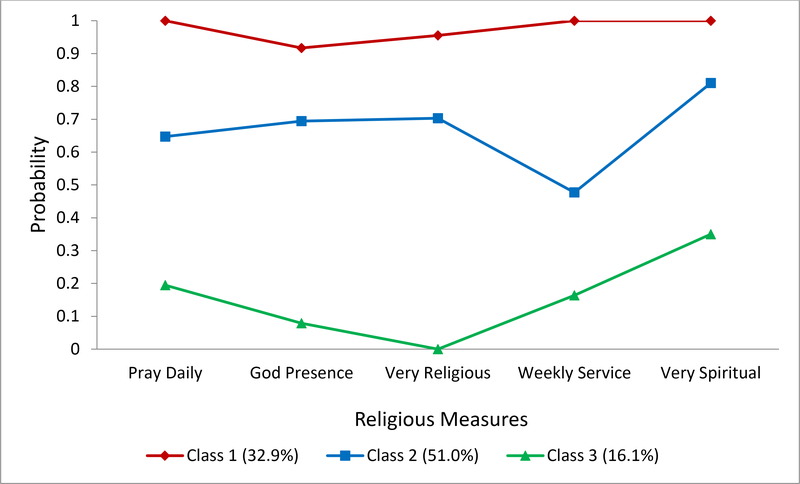
Patients were 56.1% male, 86.1% Black/African American, aged 22-77 (Mean=50.83). 75.3% were Christian. LCA identified three classes: traditionally religious (35%), privately religious (47.1%), and spiritual but not religious (17.9%). MOS-HIV mental health ( < 0.001), MOS-HIV quality of life ( = 0.014) and MOS-HIV health transition ( = 0.016) scores were significantly higher among patients who were traditionally religious. These patients were more likely to be 40+ years and Black. Patients in the privately religious group had the lowest levels of mental health and HRQoL.
Understanding how religiousness and spirituality influence HRQoL can help the medical community develop holistic, patient-centered and culturally-sensitive interventions that could improve outcomes for PLWH and potentially mitigate the impact of health disparities within the Black and LGBTQ communities.
了解宗教和精神信仰如何影响健康相关生活质量(HRQoL)对于开展全面的、以患者为中心的治疗至关重要。本研究确定了成年HIV感染者(PLWH)宗教信仰/精神信仰的不同潜在类别,以及潜在类别归属与HRQoL之间的关联。
从针对PLWH的家庭中心(FACE)预先护理计划(ACP)临床试验中的223名患者收集基线数据。患者完成了宗教信仰/精神信仰简短多维测量(改编后的BMMRS)、患者健康问卷(PHQ-9)、医学结果研究-HIV调查(MOS-HIV)和姑息治疗结果量表(POS)。通过将K类模型与(K-1)类模型进行迭代比较来确定潜在类别的最佳数量。评估了潜在类别归属、HRQoL与人口统计学特征之间的关系。
患者中男性占56.1%,黑人/非裔美国人占86.1%,年龄在22-77岁之间(平均=50.83)。75.3%为基督教徒。潜在类别分析确定了三类:传统宗教信仰者(35%)、私人宗教信仰者(47.1%)和有精神信仰但无宗教信仰者(17.9%)。传统宗教信仰者的MOS-HIV心理健康得分(<0.001)、MOS-HIV生活质量得分(=0.014)和MOS-HIV健康转变得分(=0.016)显著更高。这些患者更可能年龄在40岁及以上且为黑人。私人宗教信仰组患者的心理健康和HRQoL水平最低。
了解宗教信仰和精神信仰如何影响HRQoL有助于医学界制定全面的、以患者为中心且具有文化敏感性的干预措施,从而改善PLWH的治疗效果,并有可能减轻黑人和 LGBTQ 社区内健康差异的影响。