Som Avik, Lang Min, Yeung Tristan, Carey Denston, Garrana Sherief, Mendoza Dexter P, Flores Efren J, Li Matthew D, Sharma Amita, McDermott Shaunagh, Shepard Jo-Anne O, Little Brent P
Department of Radiology, Massachusetts General Hospital, Boston, MA, USA (A.S., M.L., S.G., D.P.M., E.J.F., M.D.L., A.S., S.M., J.A.O.S., B.P.L.); and Harvard Medical School, Boston, MA, USA (T.Y., D.C.).
Radiol Cardiothorac Imaging. 2020 Sep 10;2(5):e200276. doi: 10.1148/ryct.2020200276. eCollection 2020 Oct.
RSNA expert consensus guidelines provide a framework for reporting CT findings related to COVID-19, but have had limited multireader validation.
To assess the performance of the RSNA guidelines and quantify interobserver variability in application of the guidelines in patients undergoing chest CT for suspected COVID-19 pneumonia.
A retrospective search from 1/15/20 to 3/30/20 identified 89 consecutive CT scans whose radiological report mentioned COVID-19. One positive or two negative RT-PCR tests for COVID-19 were considered the gold standard for diagnosis. Each chest CT scan was evaluated using RSNA guidelines by 9 readers (6 fellowship trained thoracic radiologists and 3 radiology resident trainees). Clinical information was obtained from the electronic medical record.
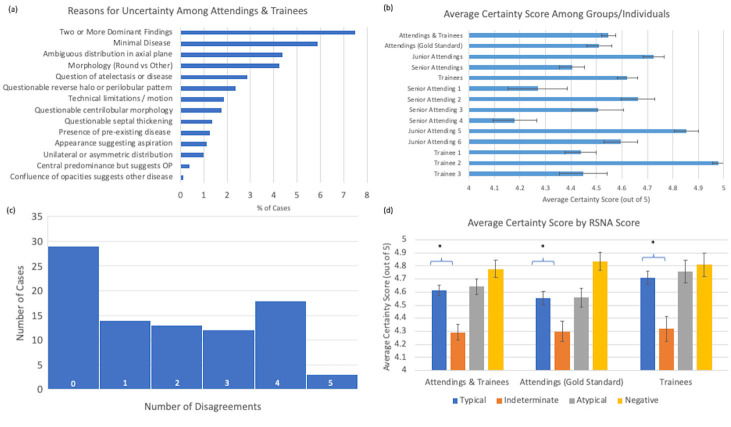
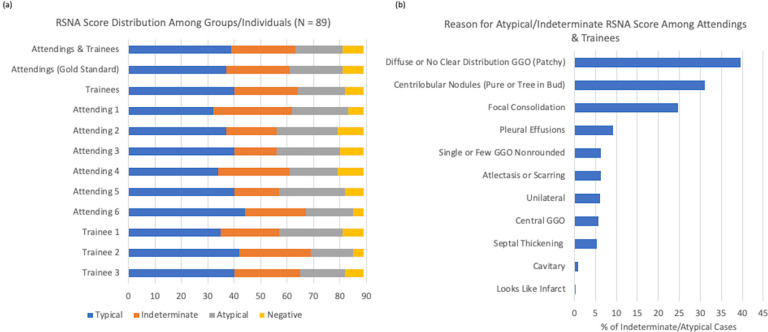
There was strong concordance of findings between radiology training levels with agreement ranging from 60 to 86% among attendings and trainees (kappa 0.43 to 0.86). Sensitivity and specificity of "typical" CT findings for COVID-19 per the RSNA guidelines were on average 86% (range 72%-94%) and 80.2% (range 75-93%), respectively. Combined "typical" and "indeterminate" findings had a sensitivity of 97.5% (range 94-100%) and specificity of 54.7% (range 37-62%). A total of 163 disagreements were seen out of 801 observations (79.6% total agreement). Uncertainty in classification primarily derived from difficulty in ascertaining peripheral distribution, multiple dominant disease processes, or minimal disease.
The "typical appearance" category for COVID-19 CT reporting has an average sensitivity of 86% and specificity rate of 80%. There is reasonable interreader agreement and good reproducibility across various levels of experience.
RSNA专家共识指南为报告与COVID-19相关的CT检查结果提供了一个框架,但多读者验证有限。
评估RSNA指南的性能,并量化在疑似COVID-19肺炎的胸部CT检查患者中应用该指南时观察者间的变异性。
回顾性检索2020年1月15日至3月30日期间连续的89例CT扫描,其放射学报告提及COVID-19。一次COVID-19核酸检测阳性或两次阴性被视为诊断的金标准。9名读者(6名接受过专科培训的胸科放射科医生和3名放射科住院医师)使用RSNA指南对每例胸部CT扫描进行评估。临床信息从电子病历中获取。
放射学培训水平之间的检查结果一致性很强,主治医师和住院医师之间的一致性范围为60%至86%(kappa值为0.43至0.86)。根据RSNA指南,COVID-19“典型”CT表现的敏感性和特异性平均分别为86%(范围72%-94%)和80.2%(范围75%-93%)。“典型”和“不确定”表现相结合的敏感性为97.5%(范围94%-100%),特异性为54.7%(范围37%-62%)。在801次观察中有163次存在分歧(总体一致性为79.6%)。分类的不确定性主要源于难以确定外周分布、多种主要疾病过程或轻微疾病。
COVID-19 CT报告的“典型表现”类别平均敏感性为86%,特异性率为80%。在不同经验水平之间存在合理的读者间一致性和良好的可重复性。