Parc Sanitari Sant Joan de Déu, Universitat de Barcelona, Fundació Sant Joan de Déu, Dr Antoni Pujades, 42, 08830 Sant Boi de Llobregat, Barcelona, Spain.
Instituto de Salud Carlos III, Centro de Investigación Biomédica en Red de Salud Mental, CIBERSAM, Monforte de Lemos 3-5, Pabellón 11, 28029 Madrid, Spain.
Eur J Prev Cardiol. 2022 May 27;29(8):1220-1232. doi: 10.1093/eurjpc/zwab015.
This study aimed at evaluating the age, sex, and country-income patterns in aortic aneurysm disease burden, analysing trends in mortality and years of life lost (YLLs), as well as their causal drivers and risk factors, using the 2017 Global Burden of Diseases, Injuries, and Risk Factors Study (GBD 2017).
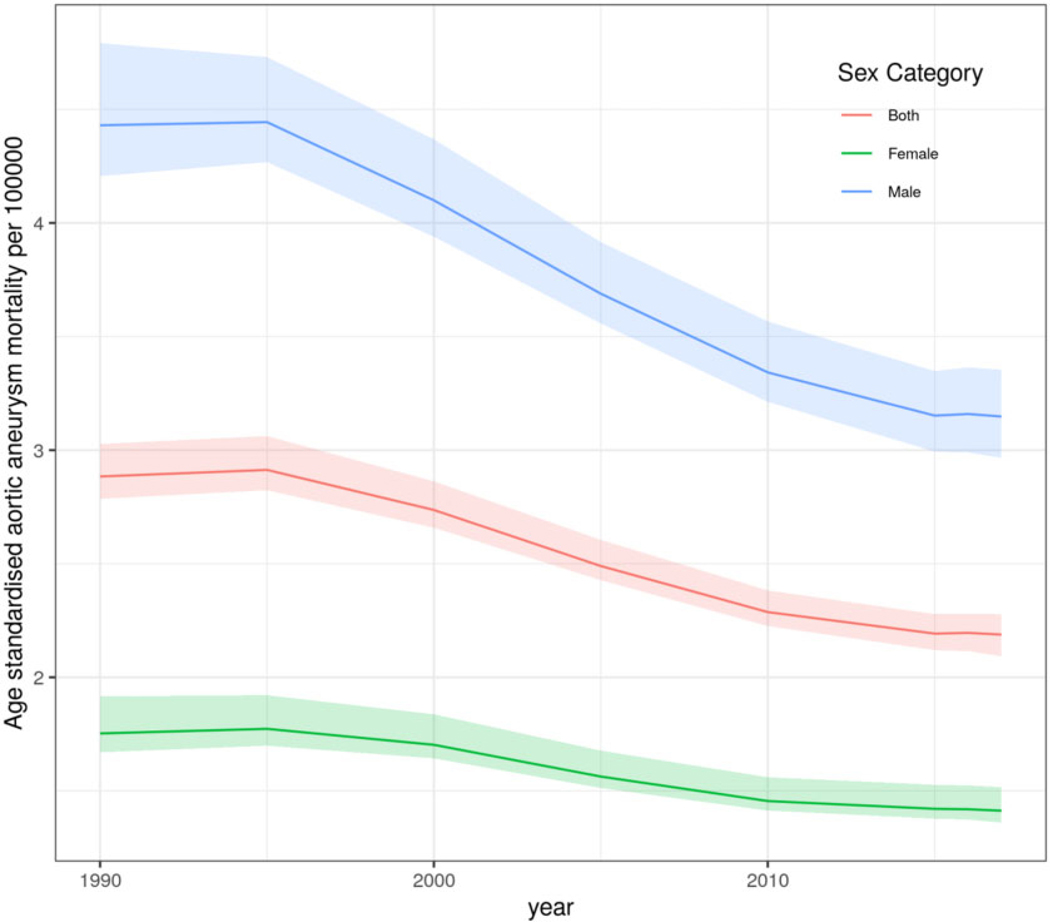
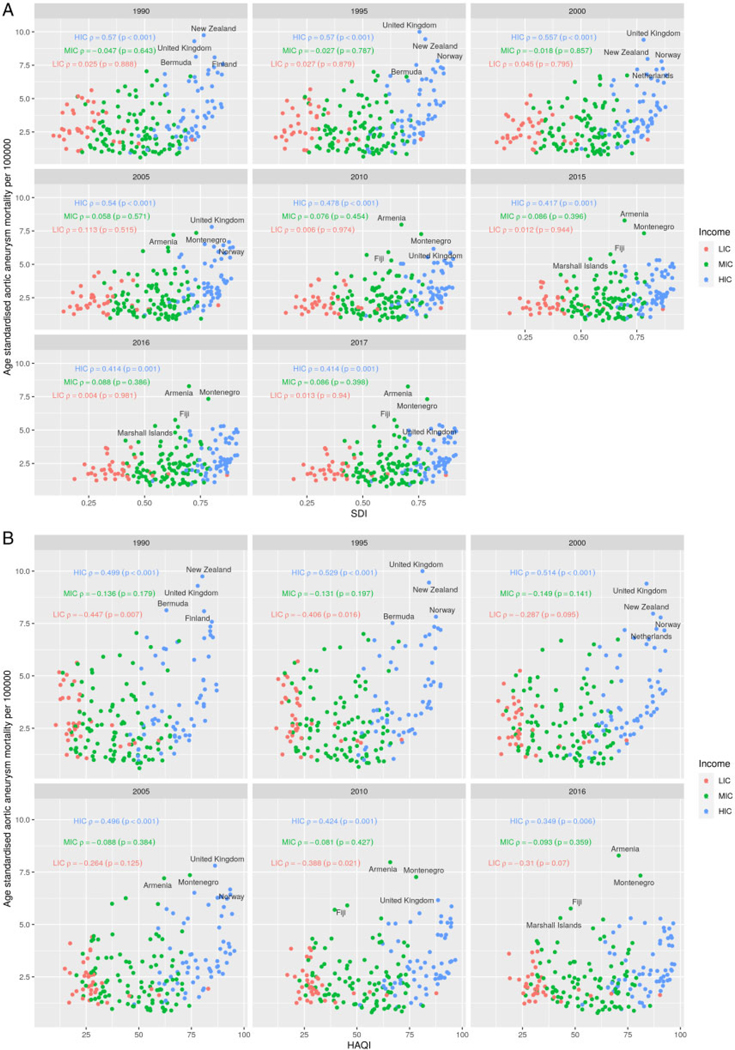
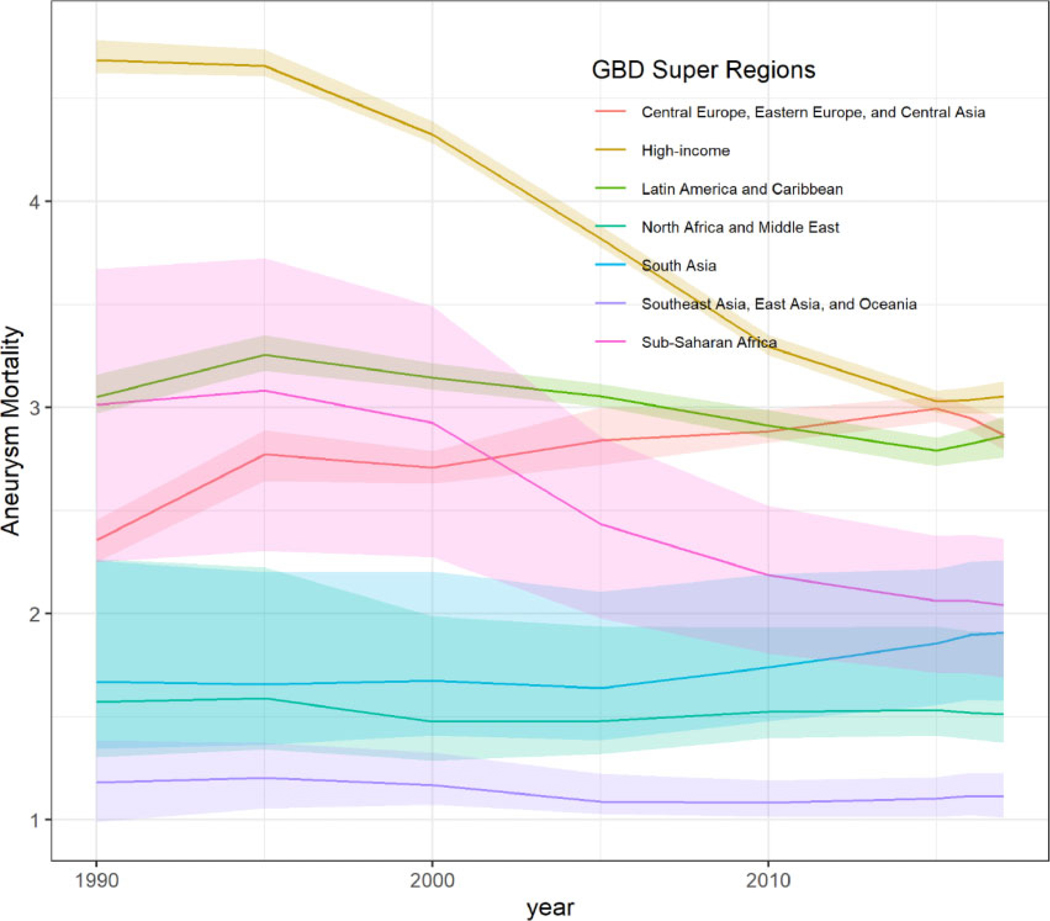
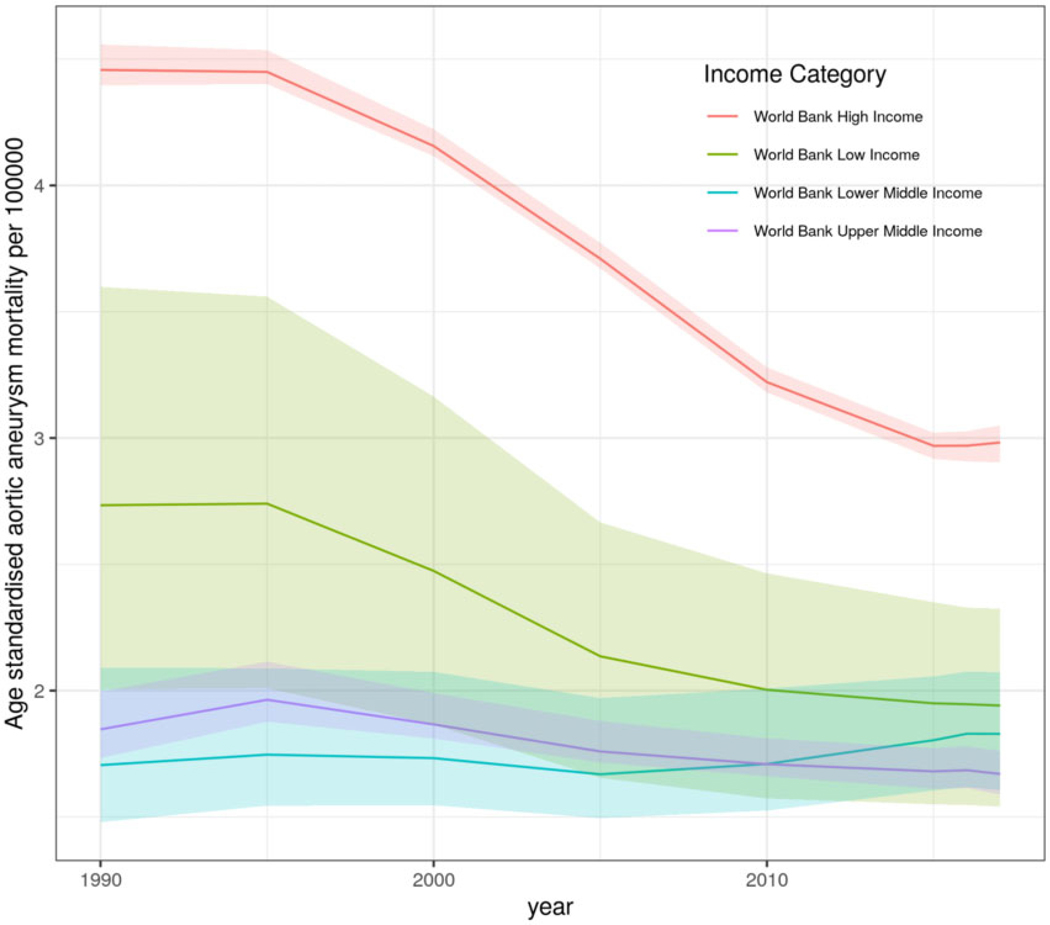
We described the temporal, global, and regional (195 countries) patterns of aortic aneurysm (thoracic and abdominal) mortality, YLLs, their drivers [sociodemographic index (SDI), healthcare access and quality index (HAQ index)] and risk factors using the GBD 1990-2017. Correlation and mixed multilevel modelling between aortic aneurysm mortality, YLLs, HAQ index and other variables were applied. From 1990 to 2017, a global declining trend in age-standardized aortic aneurysm mortality was found [2.88 deaths/100 000 (95% uncertainty intervals, UI 2.79 to 3.03) in 1990 and 2.19 deaths/100 000 (95% UI 2.09 to 2.28) in 2017]. Among high-income countries (HICs) a consistent declining Spearman's correlation between age-standardised aortic aneurysm mortality, SDI (HICs; 1990 rho: 0.57, P ≤ 0.001; 2017 rho: 0.41, P = 0.001) and HAQ index was observed (HICs; 1990 rho: 0.50, P <0.001; 2016 rho: 0.35, P = 0.006); in comparison with low- and middle-income countries where correlation trends were weak and mixed. At a global level, higher HAQ index was related with lower aortic aneurysm mortality and YLLs [mortality, coef: -0.05, 95% confidence interval (CI): -0.06, -0.04; YLLs, coef: -0.94, 95% CI: -1.17, -0.71].
Age-standardized aortic aneurysm mortality declined globally between 1990 and 2017. Globally, age-standardized aortic aneurysm mortality and YLLs were related to changes in SDI and HAQ index levels, while country-level income-related variations were also observed.
本研究旨在评估主动脉瘤疾病负担的年龄、性别和国家收入模式,分析死亡率和寿命损失年(YLL)的趋势,以及它们的因果驱动因素和风险因素,使用 2017 年全球疾病、伤害和风险因素研究(GBD 2017)。
我们使用 GBD 1990-2017 描述了全球(195 个国家)主动脉瘤(胸和腹)死亡率、YLL 及其驱动因素[社会人口指数(SDI)、医疗保健获取和质量指数(HAQ 指数)]和风险因素的时间、全球和区域模式。应用了主动脉瘤死亡率、YLL、HAQ 指数和其他变量之间的相关性和混合多水平模型。1990 年至 2017 年间,发现全球年龄标准化主动脉瘤死亡率呈下降趋势[1990 年为 2.88 例/100000(95%不确定区间,95% UI 为 2.79 至 3.03),2017 年为 2.19 例/100000(95% UI 为 2.09 至 2.28)]。在高收入国家(HICs)中,观察到年龄标准化主动脉瘤死亡率、SDI(HICs;1990 年 rho:0.57,P ≤ 0.001;2017 年 rho:0.41,P = 0.001)和 HAQ 指数之间存在一致的负相关趋势(HICs;1990 年 rho:0.50,P <0.001;2016 年 rho:0.35,P<0.001);相比之下,低收入和中等收入国家的相关性趋势较弱且混杂。在全球范围内,较高的 HAQ 指数与较低的主动脉瘤死亡率和 YLL 相关[死亡率,系数:-0.05,95%置信区间(CI):-0.06,-0.04;YLL,系数:-0.94,95% CI:-1.17,-0.71]。
1990 年至 2017 年间,全球年龄标准化主动脉瘤死亡率下降。在全球范围内,年龄标准化主动脉瘤死亡率和 YLL 与 SDI 和 HAQ 指数水平的变化有关,同时也观察到了与国家收入相关的变化。